




ResMed vs. Respironics: AHI and Variable Breathing



Re: ResMed vs. Respironics: AHI and Variable Breathing
Thinking about what I posted above, I suppose 2 OA events in the same 30-second interval could be responsible for a missing apnea in the details.
_________________
| Machine: DreamStation BiPAP® Auto Machine |
| Mask: DreamWear Nasal CPAP Mask with Headgear |
jeff
Re: ResMed vs. Respironics: AHI and Variable Breathing
Going by Velbor's chart . . .Muffy wrote: . . . The Muffpothesis offers a possible explanation why some patients may have HI Respironics < HI ResMed, namely, potential events are excluded . . .

. . . it looks to me like Respironics machines do a lot of excluding by way of filtering and hoop-jumping, as far as which events get reported as hypopneas.
One thing that pops into my head, although I don't know if it applies at all here, is that Snoredog used to say that events during ramp time were not reported to the user. If that is true, then I wonder: Is it equally true in both the summary data and detailed data? I know less than nothing about Respironics machines, so I only throw that out as a remote possibility of why the numbers might differ. I apologize if it is not relevant to the discussion at hand, which is quite a bit over my head in the technical aspects of it.jdm2857 wrote: . . . the total OA from the summary data is greater than the total number of OA events in the detail data . . .

Re: ResMed vs. Respironics: AHI and Variable Breathing
There may be some confusion re my observation that Encore Pro and EPA sometimes report more events that what is shown on the EP Sleep Therapy Flags chart. On the Sleep Therapy Daily Details page, the Sleep Therapy Flags chart is the middle one and shows "tick" marks for when the various sleep events occurred. The X-axis (horizontal axis) is shows blower hours elapsed time (not actual time-of-day).
The Sleep Therapy Flags chart is created from time-stamped 30-second intervals recorded by the Respironics machine which are transmitted via the Smartcard to Encore Pro (and Encore Viewer if EV also has such a chart). The total event counts are "correctly" reflected in the Event Indices to the right of the Flags chart. These indices, including being expanded to count the total events for the reported session duration (Thrs), are NOT sourced from the TS 30-second interval records in the EP SQL database. The indices are sourced from a separate EP SQL table that is built from a machine created session record. This session record also includes the total time in Apnea for the session. These total counts are the ones that EPA reports.
I have observed 14 differences since starting CPAP in March between the TS interval records ("tick mark" display) totals and the total counts reported by EPA (which come from the EP SQL table and which EP correctly uses/reports in its calculation of the sleep event indices).
In summary, there are two sources for EP/EPA reported/displayed sleep event counts: 1) the TS 30-second interval records, and 2) a separately reported session count that is stored in its own SQL table. EP uses the TS records to create the graphical "tick mark" display, and EP and EPA use the session counts to calculate the sleep event indices and (for EPA) the total sleep events for each category (NRAH, OA, H, FL, Snore) per session.
The Sleep Therapy Flags chart is created from time-stamped 30-second intervals recorded by the Respironics machine which are transmitted via the Smartcard to Encore Pro (and Encore Viewer if EV also has such a chart). The total event counts are "correctly" reflected in the Event Indices to the right of the Flags chart. These indices, including being expanded to count the total events for the reported session duration (Thrs), are NOT sourced from the TS 30-second interval records in the EP SQL database. The indices are sourced from a separate EP SQL table that is built from a machine created session record. This session record also includes the total time in Apnea for the session. These total counts are the ones that EPA reports.
I have observed 14 differences since starting CPAP in March between the TS interval records ("tick mark" display) totals and the total counts reported by EPA (which come from the EP SQL table and which EP correctly uses/reports in its calculation of the sleep event indices).
In summary, there are two sources for EP/EPA reported/displayed sleep event counts: 1) the TS 30-second interval records, and 2) a separately reported session count that is stored in its own SQL table. EP uses the TS records to create the graphical "tick mark" display, and EP and EPA use the session counts to calculate the sleep event indices and (for EPA) the total sleep events for each category (NRAH, OA, H, FL, Snore) per session.
_________________
| Machine: AirSense™ 10 CPAP Machine with HumidAir™ Heated Humidifier |
| Mask: ResMed AirFit™ F30 Full Face CPAP Mask with Headgear |
| Additional Comments: CPAP Auto with Min 10, Max 12, and OSCAR |
I live in my body. I know my body better than anyone else in the world. I may consult a medical professional for advice, but no one, and I do mean NO ONE tells me what I am permitted to do. - Kiralynx

Re: ResMed vs. Respironics: AHI and Variable Breathing
Darn near, it's seventh on the hierarchy:cinco777 wrote:Regarding your question as to why I believe that VB is the lowest priority in reporting sleep events rather than the highest..
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Re: ResMed vs. Respironics: AHI and Variable Breathing
jnk wrote
I have never used the ramp feature and, therefore, do not know what is or isn't reported by the machine during this "ramp" time. Neither, either, or both are possibilities. Maybe someone else has investigated this and will respond to your post and related questions.One thing that pops into my head, although I don't know if it applies at all here, is that Snoredog used to say that events during ramp time were not reported to the user. If that is true, then I wonder: Is it equally true in both the summary data and detailed data?
_________________
| Machine: AirSense™ 10 CPAP Machine with HumidAir™ Heated Humidifier |
| Mask: ResMed AirFit™ F30 Full Face CPAP Mask with Headgear |
| Additional Comments: CPAP Auto with Min 10, Max 12, and OSCAR |
I live in my body. I know my body better than anyone else in the world. I may consult a medical professional for advice, but no one, and I do mean NO ONE tells me what I am permitted to do. - Kiralynx
That's Great, But What's It Really Mean?
If we are to believe that the VB Controller works the way the patent describes, one is in "VB Mode" after exceeding an upper threshold (306):
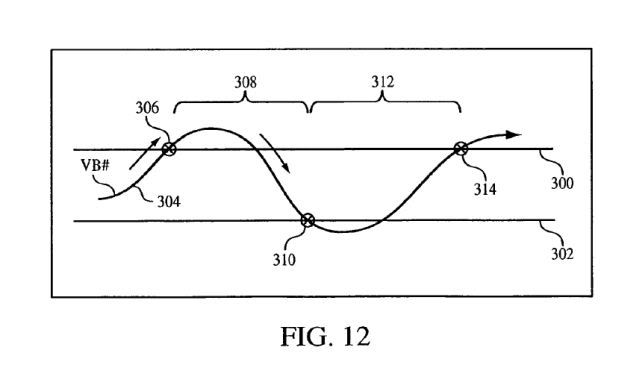
One stays in VB Mode, however, not only when VB# drops below upper threshold, but through what might be considered "normalcy" until a lower threshold is reached (310). It is this area (308) that I believe to be the area of vulnerability, when hypopneas could occur but be left unscored, whereas A10 would be in a position to score them.
While we could create an acid test for Muffpothesis (Respironics/ResMed users, HI differences and VB%), I would like to suggest a third arm to the discussion, namely, what to do with the ResMed HI "half" that heretofore is cast off as being...
being...
I don't think I heard the rationale of why it could be cast off.
Anyway, calculating all this backwards, I would suggest that the cast off ResMed HI could actually be comparable to VB-- specifically, the aforementioned "troubled wake".
In other words, an intractable HI would be strongly suggestive not of SBD, but disrupted sleep.
Muffy
One stays in VB Mode, however, not only when VB# drops below upper threshold, but through what might be considered "normalcy" until a lower threshold is reached (310). It is this area (308) that I believe to be the area of vulnerability, when hypopneas could occur but be left unscored, whereas A10 would be in a position to score them.
While we could create an acid test for Muffpothesis (Respironics/ResMed users, HI differences and VB%), I would like to suggest a third arm to the discussion, namely, what to do with the ResMed HI "half" that heretofore is cast off as being...
being...
I don't think I heard the rationale of why it could be cast off.
Anyway, calculating all this backwards, I would suggest that the cast off ResMed HI could actually be comparable to VB-- specifically, the aforementioned "troubled wake".
In other words, an intractable HI would be strongly suggestive not of SBD, but disrupted sleep.
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem

Re: ResMed vs. Respironics: AHI and Variable Breathing
I haven't seen any discussion as to why Respironics tracts VB and not ResMed...is this something we as apneics should know about and tract? Or, is this an esoteric factor that at most might affect only those with really complex SDB? If the latter then why does Respironics have it there as a layer? What is its function...data collection for some ulterior corporate research doesn't make sense in adding this layer to all devices and reeks of conspiracy theory (not that there isn;pt some rality there sometimes ). Didn't I read in the other thread that when in VB, AIs-HIs aren't scored or was it that they were not responded to (my brain's not fully back yet, I confuse easily...sorry!).
ResMed S9 range 9.8-17, RespCare Hybrid FFM
Never, never, never, never say never.
Never, never, never, never say never.
Re: ResMed vs. Respironics: AHI and Variable Breathing
Muse-Inc wrote
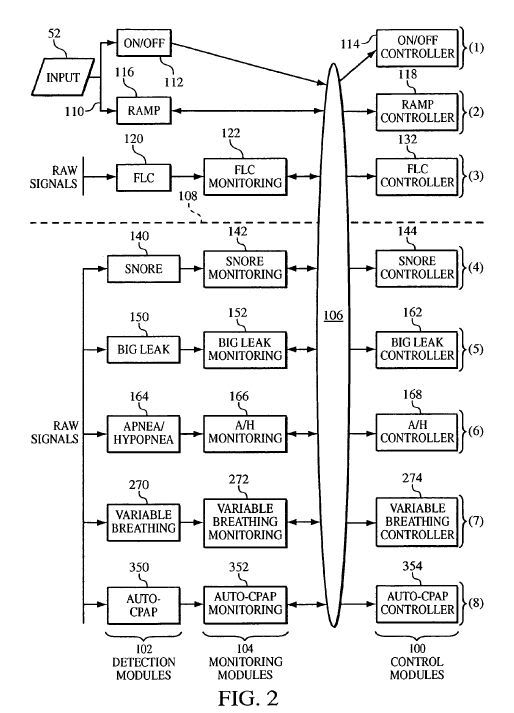
Other than being mentioned in patents, Respironics continues to be mute on the subject of VB. Various theories have been proposed and continue to be challenged and critiqued by forum members. Whether any credible answers will be forthcoming from this VB investigation is still an unknown but not for lack of trying!
Velbor and other technically curious folks on this forum are investigating the Respironics Variable Breathing (VB) "mystery". The technical objectives of this investigation include trying to determine: 1) WHY Respironics detects, records, and reports VB events, 2) WHAT is the relationship between VB events and SDB, and 3) HOW are VB events used to monitor and/or modify our CPAP sleep therapy. Of course, VB event detection and reporting may be, as some have suggested, a failed hardware and software implementation that was less costly to leave "as is" than to remove.I haven't seen any discussion as to why Respironics tracts VB and not ResMed...is this something we as apneics should know about and tract? Or, is this an esoteric factor that at most might affect only those with really complex SDB? If the latter then why does Respironics have it there as a layer? What is its function...data collection for some ulterior corporate research doesn't make sense in adding this layer to all devices and reeks of conspiracy theory (not that there isn;pt some rality there sometimes ). Didn't I read in the other thread that when in VB, AIs-HIs aren't scored or was it that they were not responded to (my brain's not fully back yet, I confuse easily...sorry!).
Other than being mentioned in patents, Respironics continues to be mute on the subject of VB. Various theories have been proposed and continue to be challenged and critiqued by forum members. Whether any credible answers will be forthcoming from this VB investigation is still an unknown but not for lack of trying!
_________________
| Machine: AirSense™ 10 CPAP Machine with HumidAir™ Heated Humidifier |
| Mask: ResMed AirFit™ F30 Full Face CPAP Mask with Headgear |
| Additional Comments: CPAP Auto with Min 10, Max 12, and OSCAR |
I live in my body. I know my body better than anyone else in the world. I may consult a medical professional for advice, but no one, and I do mean NO ONE tells me what I am permitted to do. - Kiralynx
Re: ResMed vs. Respironics: AHI and Variable Breathing
The Variable Breathing Controller was designed for use in the AutoTitration Algorithm. It's based on the principle that there are periods of disturbed breathing that should not be considered for pressure attack, particularly troubled wake and phasic REM. Trying to paraphrase the patent somewhat and make it a little more understandable:Muse-Inc wrote:What is (VB) function...
Variable Breathing Pressure Control
Once the variable breathing controller has been granted control of the pressure support system, it takes some initial action based on the action the auto-CPAP controller is taking. After this initial action, it performs an independent pressure control operation.
A prior pressure that is flat will cause the pressure delivered to the patient to remain at that level.
A prior pressure that is increasing will cause the variable breathing controller to initially decrease the pressure delivered to the patient at a rate of 0.5 cmH2O per minute. The magnitude of the decrease is dependent on the magnitude of the increase in prior pressure. The pressure decrease is intended to erase the prior pressure increase that possibly caused the variable breathing. However, the total decrease in pressure drop is limited to 2 cmH2O. After pressure decrease, the variable breathing controller holds the pressure steady.
A prior pressure that is decreasing will cause the variable breathing controller to initially increase the pressure delivered to the patient at a rate of 0.5 cmH2O per minute. The magnitude of the increase is dependent on the magnitude of the decrease in prior pressure. The pressure increase is intended to erase the prior pressure decrease that may have caused the variable breathing. However, the total increase in pressure is limited to 2 cmH2O. After pressure increase, variable breathing controller holds the pressure steady.
The pressure curve is provided for 5 minutes or until the variable breathing condition clears. Thereafter, the pressure is controlled according to the following:
The pressure is either maintained at a constant value, or it follows a decrease and hold pattern. The decision to hold the pressure or to decrease the pressure is made by comparing the current pressure with the snore treatment pressure. It is to be understood, however, that this duration can be varied over a range of durations.
If there is no snore treatment pressure stored in the system, which will be the case if the snore controller has not been activated, the pressure is held constant. If there is a snore treatment pressure, and if the current pressure is more than a predetermined amount above this snore treatment pressure, such as more than 2 cmH2O above the snore treatment pressure, the variable breathing controller decreases the pressure to a level that is a predetermined amount higher than the snore treatment pressure and holds the pressure at the lower level. The pressure decreases to the snore treatment pressure +1 cmH2O.
The duration during which pressure is provided according to the paradigms discussed above for region is set to 15 minutes or until the variable breathing condition clears. It is to be understood, however, that this 15 minute duration can be varied over a range of durations.
Muffpothesis states that since the fear of scoring events during troubled wake and phasic REM was strong enough to create exclusionary criteria, then the likelihood of there actually being events is reasonably high, and the ResMed approach (add additional criteria, such as flow limitation) would still allow events unaffected by pressure (particularly those occurring during wake) to slip through.
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Re: ResMed vs. Respironics: AHI and Variable Breathing
I guess I am still the king of variable breathing since I am still in the 40-80% and usually above 60%. My Dr. said it meant nothing and was just when your mouth puffs or mask leaks a lot. I tried everything short of super glue and never got it down although sometimes it was down in the 20's. I switched to straight CPAP at 15 and seem to do better although I still am AHI 5+ most of the time. A bad night of cpap is better than most any night without cpap!
On another note - I haven't been around much and I finally quit checking my card every morning a long time ago. I can tell when it was a bad night without checking the numbers. I still check as needed.
On another note - I haven't been around much and I finally quit checking my card every morning a long time ago. I can tell when it was a bad night without checking the numbers. I still check as needed.
MrSandman - Send me a dream...
Hey, I wanted a cool name related to sleep...
Hey, I wanted a cool name related to sleep...
Re: ResMed vs. Respironics: AHI and Variable Breathing
THANKS! Your paraphrasing was really helpful. I assume that Respironics is thinking that variable breathing MIGHT be triggered by the most recent pressure changes because when it detects VB its devices increase or decrease pressure to offset whichever pressure change might have triggered the VB -- correct? How does this align with the central nervous system's control of breathing...I must be missing something here. If we assume that the CNS controls breathing and that apneic and hypop events are mostly prevented by the identified titrated pressure and an APAP device will increase pressure in an attempt to abort a potential apnea or hypopnea event...then is Respironics assuming that a pressure change might somehow affect the CNS's control of breathing at least enough to trigger VB? This begs the question as to whether there is a CNS feedback loop affected by CPAP therapy. If pressure changes do indeed affect the regularity-consistency of breathing, this might explain why some report that an APAP's variable pressure increases their events.Muffy wrote:...Trying to paraphrase the patent somewhat and make it a little more understandable...
Events unaffected by pressure...uh, I'm a bit confused here, would these be centrals (initiated by the CNS right?) or those non-responsive (to increased pressure right?) events that Respironics reports? Are there others? I understood that apnea and hypop events were pretty much flow restrictions (with resulting desaturations) caused by narrowed or collasped airways which are eliminated by CPAP that delivers the titrated pressure to our airways...or did I miss-sleep thru something important in "Apnea 101 Basics" or is this part of "Apnea xxx Esoteria"?Muffy wrote:...Muffpothesis states that since the fear of scoring events during troubled wake and phasic REM was strong enough to create exclusionary criteria, then the likelihood of there actually being events is reasonably high, and the ResMed approach (add additional criteria, such as flow limitation) would still allow events unaffected by pressure (particularly those occurring during wake) to slip through.
Fear of scoring events begs the question why? And, the whole issue of VB--at least during sleep--begs the question of what causes it, is it affected by CPAP therapy, is it a new wrinkle in SDB, is it a factor in a person's subjective sense of well-being, does it affect SpO2, does it affect sleep architecture...all unanswered perhaps uninvestigated questions at this time.
ResMed S9 range 9.8-17, RespCare Hybrid FFM
Never, never, never, never say never.
Never, never, never, never say never.
We'll Be Right Back After These Messages...
Those are some pretty insightful observations there, MI, and beg for additional discussion! Right now, tho, I'm back on vac and using the WiFi here at the coffee shop, but I'll join in a little later.
Off to get a hefty dose of Vitamin D!
Muffy
Off to get a hefty dose of Vitamin D!
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Re: ResMed vs. Respironics: AHI and Variable Breathing
I just read this posted by -SWS in another thread:
I wonder if Respironics is concerned that pressure changes might initiate breathing changes that then might skew blood gases (not sure how variable these are) which then could conceivably initiate ongoing or prolonged periods of VB or in some with CompSDB (CompSAS?) PB. Could it be that whenever we hyperventilate (reaction to apnea or hypop events) with its skewing of blood gases (and BP), that we risk initiating additonal apneas, hypops, or even centrals with further skewing of blod gases? Could it be that Respironics is erring on the side of caution with the VB layer which backs off changes that might have initated periods of VB because of ultimate concern with blood gas skewing that might initiate repetitive loops of events?...this highly speculative thought might be baseless if VB does not have the potential to affect blood gases.Periodic breathing's preliminary hyperventilation stage is believed to sufficiently skew dynamic blood-gas values, causing those interrelated central apneas and/or hypopneas to occur.
ResMed S9 range 9.8-17, RespCare Hybrid FFM
Never, never, never, never say never.
Never, never, never, never say never.
Re: ResMed vs. Respironics: AHI and Variable Breathing
No, I believe the VB algorithm is only concerned with troubled wake and phasic REM, as the algorithm searches for "erratic" breathing in order to try to identify those states. Pressure increases are neither needed nor wanted during those states.Muse-Inc wrote: Could it be that Respironics is erring on the side of caution with the VB layer which backs off changes that might have initated periods of VB because of ultimate concern with blood gas skewing that might initiate repetitive loops of events?...
I don't believe "repetitive loops of events" would fit that bill, rather, they would/could/should be picked up as "periodic" breathing (as long as you have the Respironics AutoSV and the ASV algorithm).
Muffy
________________________________
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem
Machine: Dell Dimension 8100
Mask: 3M N-95 (during flu season)
Humidifier: Avoided, tends to make me moldy
Software: XP Pro
Additional Comments: You can't find a solution when you don't know the problem

OT: Mr Sandman
Mr Sandman,
I'm rather curious as to why you chose an avatar of Pissing on the USA. Its more than a bit offensive. I've tried to avoid commenting on it - but it does get to me each time I see one of your posts.
I'm rather curious as to why you chose an avatar of Pissing on the USA. Its more than a bit offensive. I've tried to avoid commenting on it - but it does get to me each time I see one of your posts.
_________________
| Mask: Quattro™ FX Full Face CPAP Mask with Headgear |
| Additional Comments: PR SystemOne BPAP Auto w/Bi-Flex & Humidifier - EncorePro 2.2 Software - Contec CMS-50D+ Oximeter - Respironics EverFlo Q Concentrator |
Women are Angels. And when someone breaks our wings, we simply continue to fly.....on a broomstick. We are flexible like that.
My computer says I need to upgrade my brain to be compatible with its new software.
My computer says I need to upgrade my brain to be compatible with its new software.