






Palerider your response came across as extremely patronising. I'm not sure how your surprised by the tone of his response.....palerider wrote:well, since you're of such delicate sensibilities that a straightforward factual reply hurts your little feelers, I'll refrain from reading anything else you write, or ask for help with, lest I wound you again.tl424 wrote:No need to be an asshole, I'm asking a fairly innocent question, not hurting anybody..
ta, and good luck with your treatment.
Full face masks, from a viewpoint of an engineering student
Re: Full face masks, from a viewpoint of an engineering student
_________________
| Machine: DreamStation Auto CPAP Machine |
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
-
Jay Aitchsee

- Posts: 2936
- Joined: Sun May 22, 2011 12:47 pm
- Location: Southwest Florida
Re: Full face masks, from a viewpoint of an engineering student
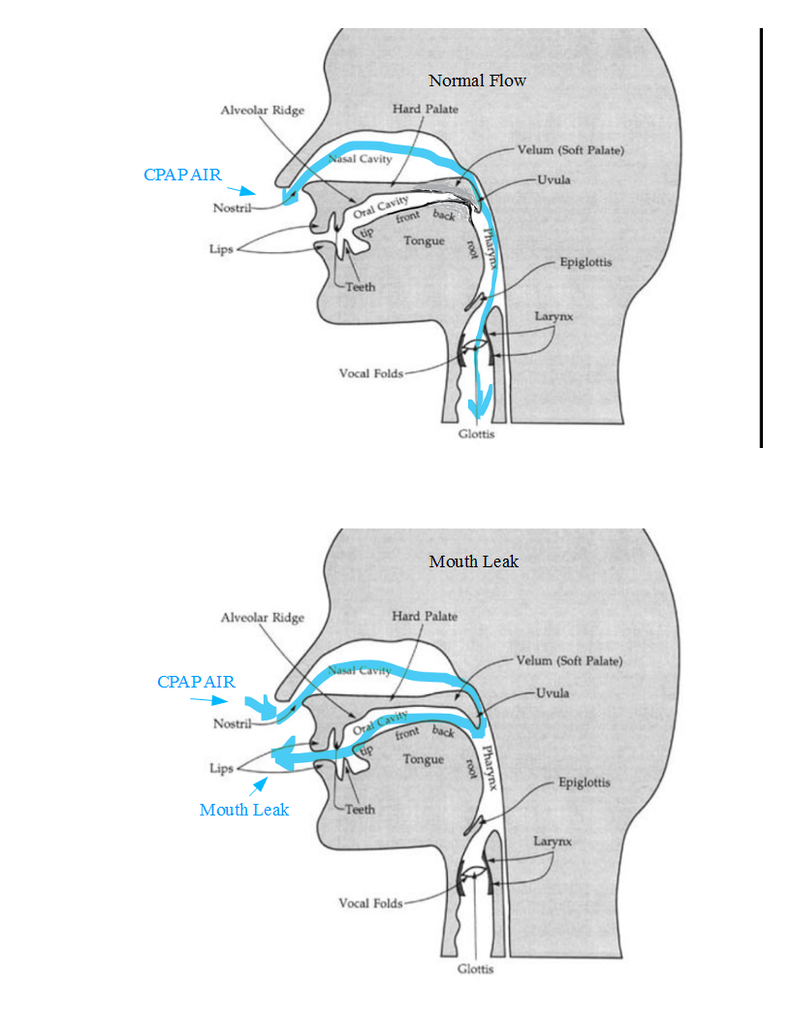
Hey TL, your question has been answered above, it's the pressure differential between the airway and room air (ambient) that splints the airway open. But that pressure differential could be lost if the velopharyngeal sphincter is open and the mouth is open to ambient. Applying therapy pressure to the mouth as well as the nose prevents the loss of therapy pressure in the airway should the velopharyngeal sphincter not seal.
The graphic below illustrates the airflow of a mouth leak with a velopharyngeal failure. I think it is easy to see how a FFM would compensate.
viewtopic.php?f=1&t=112758&p=1085906#p1085906
The graphic below illustrates the airflow of a mouth leak with a velopharyngeal failure. I think it is easy to see how a FFM would compensate.
viewtopic.php?f=1&t=112758&p=1085906#p1085906
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: S9 Auto, P10 mask, P=7.0, EPR3, ResScan 5.3, SleepyHead V1.B2, Windows 10, ZEO, CMS50F, Infrared Video |

Re: Full face masks, from a viewpoint of an engineering student
well, if you're too stupid to use the foe list...Goofproof wrote:Could the rest of us get a little of the same treatment? If so, thanks in advance. Jim
Get OSCAR
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Re: Full face masks, from a viewpoint of an engineering student
who's surprised?K34RT wrote:Palerider your response came across as extremely patronising. I'm not sure how your surprised by the tone of his response.....
I just don't have time to waste on people like that.
Get OSCAR
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
-
chunkyfrog

- Posts: 34544
- Joined: Mon Jul 12, 2010 5:10 pm
- Location: Nowhere special--this year in particular.
Re: Full face masks, from a viewpoint of an engineering student
Some of us are old enough to remember iron lungs.
The pressure differential in both cases is between the air passage OPENINGS
and the external atmospheric pressure on the chest wall.
You can either raise the pressure at the nose and/or mouth; or reduce the air pressure around the chest.
The pressure differential in both cases is between the air passage OPENINGS
and the external atmospheric pressure on the chest wall.
You can either raise the pressure at the nose and/or mouth; or reduce the air pressure around the chest.
_________________
| Mask: AirFit™ P10 For Her Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Airsense 10 Autoset for Her |
Re: Full face masks, from a viewpoint of an engineering student
The human body is generally solid, although we have plenty of fluids (and gasses) in it. The point is, with the exception of some cavities containing gasses, our body is incompressible. The oral/nasal cavity is supported by bones and although it can give a bit, it can be thought of as a solid. Thus, the pressure exerted by the forced air acts to push the soft tissue lining those cavities against a solid foundation, and therefore does not depend on the ambient (atmospheric) pressure in the room. The role of ambient pressure is very minute - it can influence the blood pressure by varying the constriction of peripheral blood vessels and redistributing the inner pressure, but you need to go from mount Everest to a deep dive to feel any effects.
As an example, the reason why scuba divers need higher pressure the deeper they go (keeping it equal to ambient) is to aid with the expansion of their lungs (makes it easier/possible to inhale). This pressure being much higher than any CPAP can deliver, it does have a profound effect on tissues, mostly by dissolving more air into the blood (not counting unusual incidents, such as barotrauma). The increased pressure on your soft tissues is felt but tolerated. The connections between the various air cavities (e.g., the Eustachian tubes) equalize it so that you only have compression of soft tissue against soild bone or strong muscle. But beware if you have an infection and some of those passages are blocked and you can't clear the ears (equalize the pressure) as you descend - it feels like it would explode (and it will) and you simply can't dive.
There are different kinds of masks but in the end what matters is the pressure delivered to the oral/nasal cavity. Unfortunately, it is not as simple as the machine would make it seem. The difference is not caused as much by the inlet mechanism (nose/mouth) but by the structure of the those cavities. But most of all, it is influenced by the breathing dynamics - even with constant CPAP delivery, the pressure inside the cavities varies wildly as we breathe. What is often forgotten when talking about the efficiency of a CPAP therapy is the actual air flow produced influencing the therapeutic pressure: for a given machine-set pressure, the higher the flow - the lower the actual pressure on the tissues. The tremendous complexity of this dynamic is a major reason why CPAP treatment remains a mostly empirical discipline. Which is why forums like this one are often more useful than sleep professionals' advice.
McSleepy
As an example, the reason why scuba divers need higher pressure the deeper they go (keeping it equal to ambient) is to aid with the expansion of their lungs (makes it easier/possible to inhale). This pressure being much higher than any CPAP can deliver, it does have a profound effect on tissues, mostly by dissolving more air into the blood (not counting unusual incidents, such as barotrauma). The increased pressure on your soft tissues is felt but tolerated. The connections between the various air cavities (e.g., the Eustachian tubes) equalize it so that you only have compression of soft tissue against soild bone or strong muscle. But beware if you have an infection and some of those passages are blocked and you can't clear the ears (equalize the pressure) as you descend - it feels like it would explode (and it will) and you simply can't dive.
There are different kinds of masks but in the end what matters is the pressure delivered to the oral/nasal cavity. Unfortunately, it is not as simple as the machine would make it seem. The difference is not caused as much by the inlet mechanism (nose/mouth) but by the structure of the those cavities. But most of all, it is influenced by the breathing dynamics - even with constant CPAP delivery, the pressure inside the cavities varies wildly as we breathe. What is often forgotten when talking about the efficiency of a CPAP therapy is the actual air flow produced influencing the therapeutic pressure: for a given machine-set pressure, the higher the flow - the lower the actual pressure on the tissues. The tremendous complexity of this dynamic is a major reason why CPAP treatment remains a mostly empirical discipline. Which is why forums like this one are often more useful than sleep professionals' advice.
McSleepy
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Previous machine: ResMed S9 VPAP Auto 25 BiLevel. Mask: Breeze with dilator pillows. Software: ResScan ver. 5.1 |
ResMed AirCurve 10 VAuto; Puritan-Bennett Breeze nasal pillow mask; healthy, active, middle-aged man; tall, athletic build; stomach sleeper; on CPAP since 2003; lives @ 5000 ft; surgically-corrected deviated septum and turbinates; regular nasal washes
Re: Full face masks, from a viewpoint of an engineering student
no.McSleepy wrote:Thus, the pressure exerted by the forced air acts to push the soft tissue lining those cavities against a solid foundation, and therefore does not depend on the ambient (atmospheric) pressure in the room.
no. the air flow in your breathing passages is purely a function of your normal respiration, and is the same with or without cpap. increased cpap pressure does not result in faster airflow in your respiratory system.McSleepy wrote: What is often forgotten when talking about the efficiency of a CPAP therapy is the actual air flow produced influencing the therapeutic pressure: for a given machine-set pressure, the higher the flow - the lower the actual pressure on the tissues.
though I'd be quite interested in the actual mathematical proof you're using to back up your claims.
Get OSCAR
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.

Re: Full face masks, from a viewpoint of an engineering student
palerider wrote:
though I'd be quite interested in the actual mathematical proof you're using to back up your claims.
****?*** totally unsure of the etiquette of being invisable ?
(please don't QUOTE *me* on that?)
...but I loved this invitation by PaleRider.
I am so hoping MATHis coming?
_________________
| Machine: ResMed AirSense™ 10 AutoSet™ CPAP Machine with HumidAir™ Heated Humidifier |
| Mask: DreamWear Nasal CPAP Mask with Headgear - Fit Pack (All Cushions Included with Medium Frame) |
| Additional Comments: Resmed 10 AirSense |
Began XPAP May 2016. Autoset Pressure min. 8 / max 15. Ramp off. ERP set at 2. No humidity. Sleepyhead software installed and being looked at daily, though only beginning to understand the data.
-
chunkyfrog
- Posts: 34544
- Joined: Mon Jul 12, 2010 5:10 pm
- Location: Nowhere special--this year in particular.
Re: Full face masks, from a viewpoint of an engineering student
Actually, PR is (cough, cough) correct.
The cpap blows air into a confined space (you), when it STOPS moving, having created pressure,
but props the weak tissues open with that PRESSURE.
We continue to breathe, in and out, at the same rate as if we did not have an obstruction.
This is why using cpap can be so comfortable that we may think it has stopped running.
The cpap blows air into a confined space (you), when it STOPS moving, having created pressure,
but props the weak tissues open with that PRESSURE.
We continue to breathe, in and out, at the same rate as if we did not have an obstruction.
This is why using cpap can be so comfortable that we may think it has stopped running.
_________________
| Mask: AirFit™ P10 For Her Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Airsense 10 Autoset for Her |
-
ChicagoGranny

- Posts: 15388
- Joined: Sun Jan 29, 2012 1:43 pm
- Location: USA
Re: Full face masks, from a viewpoint of an engineering student
1. Maybe you meant to say breathing exclusively through the nose requires a lower CPAP pressure than breathing with mouth open?grayghost4 wrote:... a nasal mask seem to work at a lower pressure than the full-face mask. ...
2. From my personal experience, #1 is clearly correct.
3. I believe it is not breathing through the mouth, per se, that causes a need for higher pressure. Instead, when the mouth opens, the jaw tends to drop backwards slightly. This causes a narrowing of the airway and makes the airway more subject to collapse.
Re: Full face masks, from a viewpoint of an engineering student
Do you mathematically prove anything you say? Or just ask others to do it? Plus, this is not mathematics, it's physics. And basic physics, at that. The basis for my conclusions are rather fundamental and I'll lay out some of them here, but I don't intend to engage in a mindless argument. I don't even understand the statement you made, so I'm not really answering it, just explaining mine. This isn't about pride and I'm secure enough to not want to waste my time in proving myself. Maybe the student who asked the question would benefit from it, though, so here are the basics.palerider wrote:no.McSleepy wrote:Thus, the pressure exerted by the forced air acts to push the soft tissue lining those cavities against a solid foundation, and therefore does not depend on the ambient (atmospheric) pressure in the room.
no. the air flow in your breathing passages is purely a function of your normal respiration, and is the same with or without cpap. increased cpap pressure does not result in faster airflow in your respiratory system.McSleepy wrote: What is often forgotten when talking about the efficiency of a CPAP therapy is the actual air flow produced influencing the therapeutic pressure: for a given machine-set pressure, the higher the flow - the lower the actual pressure on the tissues.
though I'd be quite interested in the actual mathematical proof you're using to back up your claims.
Pressure is a force that is distributed over a rigid surface. Only in the static case (no motion) is it evenly distributed, balanced and its value - constant, but it is, nonetheless, defined at all times. In the static case, if you apply a known pressure to a chamber (e.g., where the CPAP sensor is) connected to another chamber (your oral/nasal cavity) and want to know the pressure on the surface of that cavity, then you don't need to know anything else - that's the same pressure everywhere. The static case is realized when you have a rigid boundary and no change in mass (constant volume and no addition or subtraction of air; temperature, too, but let's not get into thermodynamics). As an example, If you connect the CPAP machine to a glass bottle, you can rest assured that the pressure inside would be exactly the same as the gauge reads and would not be affected at all by ambient pressure as the latter is fully balanced by the rigid body of the bottle (and so is the inner pressure, delivered by the CPAP); they are simply not allowed to interact with each other. The model of the human oral/nasal cavity is close enough to the bottle (the skull is rigid) when you are not breathing (between breaths). In the dynamic case the pressure over the boundaries can vary from, say, the inlet pressure, and across the boundary itself, but it still would not be affected by the pressure outside the boundaries, as long as those are rigid, for the same reasons. If the boundaries were not rigid, then there would be some variation from yield but unless those boundaries vary a lot, it would not be significant. In this case we may not know the exact value of the pressure inside the chamber (cavity) but the latter is still not significantly affected by ambient pressure because none of the parameters are influenced by it. Now, I need to clarify something else. If we were talking about the measurement of the pressure values, we'd need to specify whether we are talking about absolute or relative pressure readings. The reading that the CPAP machine uses is a relative ("gauge") pressure, which is referenced to ambient, but the discussion has been about the effect of the physical conduits (masks, nose or mouth inlet), excluding the source, thus I have been discussing from an absolute standpoint; how you measure that is a different topic.
Looking at pressure variations in the dynamic case, though, it gets quite complicated. There are multiple aspects of it. One is if the boundaries are moving (e.g., lungs/diaphragm expanding and contracting), but since the oral/nasal cavities are on the conduit and not the reservoir, what matters is the flow of air. As you inhale and exhale the air flows quite briskly in and out through the air passages. And the pressure varies widely with the flow. I'm not going to get into details about the Bernoulli's principle and the related Venturi effect (you can look it up), but as it relates to air/CPAP, it states that the pressure over the walls of a conduit (a more or less coherent flow field) varies in proportion (quadratic) to the flow speed. Thus, each narrowing of the conduit represents a drop in pressure. A person with a lesser section of their air passage where the soft tissue needs support by the CPAP would have lesser pressure, and thus - support - than a person with a larger section, at the same pressure settings delivered by the CPAP machine. The compressibility of air makes this more complicated, but what really makes it complicated is the large variations in time of that section within the same person: head/jaw/tongue position, swelling of tissue, etc., all make it so that the pressure where it matters varies significantly from what the machine delivers. Add to that a variety of other effects, such as the throttling of the airflow by the mouth/tongue opening, and nose structure (for nasal masks; deviated septum and enlarged turbinates are a good example), which act like pressure regulators before the airflow has reached the soft tissues, and you see how the pressure readings of the machine can be quite arbitrary. Luckily, it's all empirical and CPAP users figure it out one way or another. Also, some people are affected more than others. The aforementioned nasal-passage blockages are a big factor for some, while those with nice, open air-passages don't really feel those effects. I know I didn't have any such problems and could use much lower pressures when I tried using an oral mask (Oracle; wish I could be using it), but are very sensitive to variations, and use very high pressures with my nasal-pillow mask.
I hope this makes it clearer.
McSleepy
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Previous machine: ResMed S9 VPAP Auto 25 BiLevel. Mask: Breeze with dilator pillows. Software: ResScan ver. 5.1 |
ResMed AirCurve 10 VAuto; Puritan-Bennett Breeze nasal pillow mask; healthy, active, middle-aged man; tall, athletic build; stomach sleeper; on CPAP since 2003; lives @ 5000 ft; surgically-corrected deviated septum and turbinates; regular nasal washes
Re: Full face masks, from a viewpoint of an engineering student
you're the one that came up with the theory that the pressure in the airway is significantly (otherwise, why bother bringing it up?) reduced by the act of breathing, and further erroneously implied that the pressure setting of the cpap had some relation to that. hence my request that you provide some justification for your specious claim.McSleepy wrote:Do you mathematically prove anything you say?
and if one doesn't use math to calculate the effects of physics, then there must be a lot of confused physicists out there.McSleepy wrote:Plus, this is not mathematics, it's physics. And basic physics, at that.
I don't know about YOUR head, but mine isn't filled with air, and the majority of my respiratory system is not encased in bone. not my mouth, not my throat, not most of my trachea, while my lungs are caged, the enclosure isn't rigid.McSleepy wrote:The model of the human oral/nasal cavity is close enough to the bottle (the skull is rigid)
ah, but you brought it up and alleged that there's a significant effect, without any evidence as to the magnitude of that significance. how much? a cm/h2o? less? more? so far, you've just tossed out a concept, which, of course, in THEORY is correct, but is there any practical significance to the pressure drop?McSleepy wrote: As you inhale and exhale the air flows quite briskly in and out through the air passages. And the pressure varies widely with the flow. I'm not going to get into details about the Bernoulli's principle and the related Venturi effect (you can look it up),
your theory might have some validity, except for the fact that people are titrated for effective pressure *at the machine* not in their throats, so any pressure drop along the walls of their airway due to respiration is irrelevant. if a pressure transducer were inserted into the airway and that pressure was what was used to then calculate the settings of the cpap, your ideas might have some merit in the real world.McSleepy wrote:but as it relates to air/CPAP, it states that the pressure over the walls of a conduit (a more or less coherent flow field) varies in proportion (quadratic) to the flow speed. Thus, each narrowing of the conduit represents a drop in pressure. A person with a lesser section of their air passage where the soft tissue needs support by the CPAP would have lesser pressure, and thus - support - than a person with a larger section, at the same pressure settings delivered by the CPAP machine.
as do I.McSleepy wrote:I hope this makes it clearer.
Get OSCAR
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Re: Full face masks, from a viewpoint of an engineering student
Not a single valid point. Why don't you try to state something useful and prove it, to show us how it's done? Or you never make statements, just try (unsuccessfully) to disprove others'? For anyone who has any idea of physics, what I explained would be quite clear. For example, the significance of what I described is clearly seen in the principles of the Venturi effect, in the quadratic nature of the dependence of the pressure on velocity (and velocity is directly proportional to section). I'm not going to waste time presenting calculations for something that obvious. A small change in section (10%) will translate to a larger (20%) change in pressure. That's between 14 and 17 cm H2O, and can happen in minutes, during the night.palerider wrote:you're the one that came up with the theory that the pressure in the airway is significantly (otherwise, why bother bringing it up?) reduced by the act of breathing, and further erroneously implied that the pressure setting of the cpap had some relation to that. hence my request that you provide some justification for your specious claim.McSleepy wrote:Do you mathematically prove anything you say?
and if one doesn't use math to calculate the effects of physics, then there must be a lot of confused physicists out there.McSleepy wrote:Plus, this is not mathematics, it's physics. And basic physics, at that.
I don't know about YOUR head, but mine isn't filled with air, and the majority of my respiratory system is not encased in bone. not my mouth, not my throat, not most of my trachea, while my lungs are caged, the enclosure isn't rigid.McSleepy wrote:The model of the human oral/nasal cavity is close enough to the bottle (the skull is rigid)
ah, but you brought it up and alleged that there's a significant effect, without any evidence as to the magnitude of that significance. how much? a cm/h2o? less? more? so far, you've just tossed out a concept, which, of course, in THEORY is correct, but is there any practical significance to the pressure drop?McSleepy wrote: As you inhale and exhale the air flows quite briskly in and out through the air passages. And the pressure varies widely with the flow. I'm not going to get into details about the Bernoulli's principle and the related Venturi effect (you can look it up),
your theory might have some validity, except for the fact that people are titrated for effective pressure *at the machine* not in their throats, so any pressure drop along the walls of their airway due to respiration is irrelevant. if a pressure transducer were inserted into the airway and that pressure was what was used to then calculate the settings of the cpap, your ideas might have some merit in the real world.McSleepy wrote:but as it relates to air/CPAP, it states that the pressure over the walls of a conduit (a more or less coherent flow field) varies in proportion (quadratic) to the flow speed. Thus, each narrowing of the conduit represents a drop in pressure. A person with a lesser section of their air passage where the soft tissue needs support by the CPAP would have lesser pressure, and thus - support - than a person with a larger section, at the same pressure settings delivered by the CPAP machine.
as do I.McSleepy wrote:I hope this makes it clearer.
McSleepy
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Previous machine: ResMed S9 VPAP Auto 25 BiLevel. Mask: Breeze with dilator pillows. Software: ResScan ver. 5.1 |
ResMed AirCurve 10 VAuto; Puritan-Bennett Breeze nasal pillow mask; healthy, active, middle-aged man; tall, athletic build; stomach sleeper; on CPAP since 2003; lives @ 5000 ft; surgically-corrected deviated septum and turbinates; regular nasal washes
Re: Full face masks, from a viewpoint of an engineering student
you're the one that started this, making unfounded comments, and when asked to back them up, instead of doing so, just throw out a wall of text to try and confuse people.McSleepy wrote:Not a single valid point. Why don't you try to state something useful and prove it, to show us how it's done? Or you never make statements, just try (unsuccessfully) to disprove others'? For anyone who has any idea of physics, what I explained would be quite clear. For example, the significance of what I described is clearly seen in the principles of the Venturi effect, in the quadratic nature of the dependence of the pressure on velocity (and velocity is directly proportional to section). I'm not going to waste time presenting calculations for something that obvious. A small change in section (10%) will translate to a larger (20%) change in pressure. That's between 14 and 17 cm H2O, and can happen in minutes, during the night.
McSleepy
I'm aware of the venturi effect, and bernoulli's principle, what I'm challenging you to do is back up your comments with some actual data, showing whether your theory holds water, or if the effects, in practice, are insignificant. you made the allegations, back them up, if you can.
Get OSCAR
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Accounts to put on the foe list: dataq1, clownbell, gearchange, lynninnj, mper!?, DreamDiver, Geer1, almostadoctor, sleepgeek, ajack, stom, mogy, D.H., They often post misleading, timewasting stuff.
Re: Full face masks, from a viewpoint of an engineering student
And I have - everything is backed up by a solid explanation. For those who are capable of understanding it. I'm not going to take extra time to go down to middle-school level science, I have better things to do than hang on message boards all day.palerider wrote:you're the one that started this, making unfounded comments, and when asked to back them up, instead of doing so, just throw out a wall of text to try and confuse people.McSleepy wrote:Not a single valid point. Why don't you try to state something useful and prove it, to show us how it's done? Or you never make statements, just try (unsuccessfully) to disprove others'? For anyone who has any idea of physics, what I explained would be quite clear. For example, the significance of what I described is clearly seen in the principles of the Venturi effect, in the quadratic nature of the dependence of the pressure on velocity (and velocity is directly proportional to section). I'm not going to waste time presenting calculations for something that obvious. A small change in section (10%) will translate to a larger (20%) change in pressure. That's between 14 and 17 cm H2O, and can happen in minutes, during the night.
McSleepy
I'm aware of the venturi effect, and bernoulli's principle, what I'm challenging you to do is back up your comments with some actual data, showing whether your theory holds water, or if the effects, in practice, are insignificant. you made the allegations, back them up, if you can.
McSleepy
_________________
| Machine: AirCurve™ 10 VAuto BiLevel Machine with HumidAir™ Heated Humidifier |
| Additional Comments: Previous machine: ResMed S9 VPAP Auto 25 BiLevel. Mask: Breeze with dilator pillows. Software: ResScan ver. 5.1 |
ResMed AirCurve 10 VAuto; Puritan-Bennett Breeze nasal pillow mask; healthy, active, middle-aged man; tall, athletic build; stomach sleeper; on CPAP since 2003; lives @ 5000 ft; surgically-corrected deviated septum and turbinates; regular nasal washes