





Its been a long journey trying to figure out how to lower my AHI from double digits. I started in Nov 2003 on a straight pressure machine set at 11. After joining this board I decided that I wanted more info on my nitely events. After much hassle, I got at remstar auto with c-flex and humidifier. I soon discovered that a 11 setting was doing very little-I was having cluster apneas and my AHI was thru the roof. With the help of Restedgal and SWS, we tried just about every setting, but couldn't get consistenly below double digits AHI. They suggested a 420e which has command on apnea feature. The remstar was taking its sweet time responding to my clusters, while the 420e shoots right up there. Well, funny thing-my apneas were reduced, but hypopneas increased. But it was still an improvement. Tho not enough for me. Then I tried Benadryl at nite which helped some more. Then the BIG BREAKTHRU. They suggested that I might have GERD even tho I have NO symptoms. I finally so ok, lets try it. VERY skeptical. I started taking 1 Prilosec every morning. Bingo! My AHI plummeted to between 3-5.one nite I had 0 apneas! I guess this coincides with an article I just read about "silent" GERD and OSA.A HUGE THANKS to Restedgal ,SWS and others who have helped me.
SUCCESS AT LAST-GERD,420E, PRILOSEC AND BENADRYL


2 posts
• Page 1 of 1
SUCCESS AT LAST-GERD,420E, PRILOSEC AND BENADRYL
Pain is temporary, quitting lasts forever. Lance Armstrong
-
Guest
-
snork2
420e Rocks!
the 420E works so much better than a Remstar for me also. The 420E just seems to be more responsive. I turned off IFl1.
And I used some pretty drastic surgery to get my nose working, instead of the benadryl, which is sort of the same idea.
I do use melatonin and that seems to make a difference too.
Snork1
And I used some pretty drastic surgery to get my nose working, instead of the benadryl, which is sort of the same idea.
I do use melatonin and that seems to make a difference too.
Snork1
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
loonlvr, I'm so glad your treatment has smoothed out. Your success is entirely due to SWS's great detective work as well as your determination to hang in there and keep trying to get to the bottom of the mystery of your wild clusters of events. I just passed the thoughts along...and marveled at the way you two solved it.
Very, very happy for you!! Thanks for posting about what you did. You may be helping any number of people out there who are still struggling with their treatment and have not considered undiagnosed or "silent" acid reflux. Many have reported that CPAP treatment cleared up their GERD symptoms. But for others GERD apparently can interfere with getting good CPAP treatment at all.
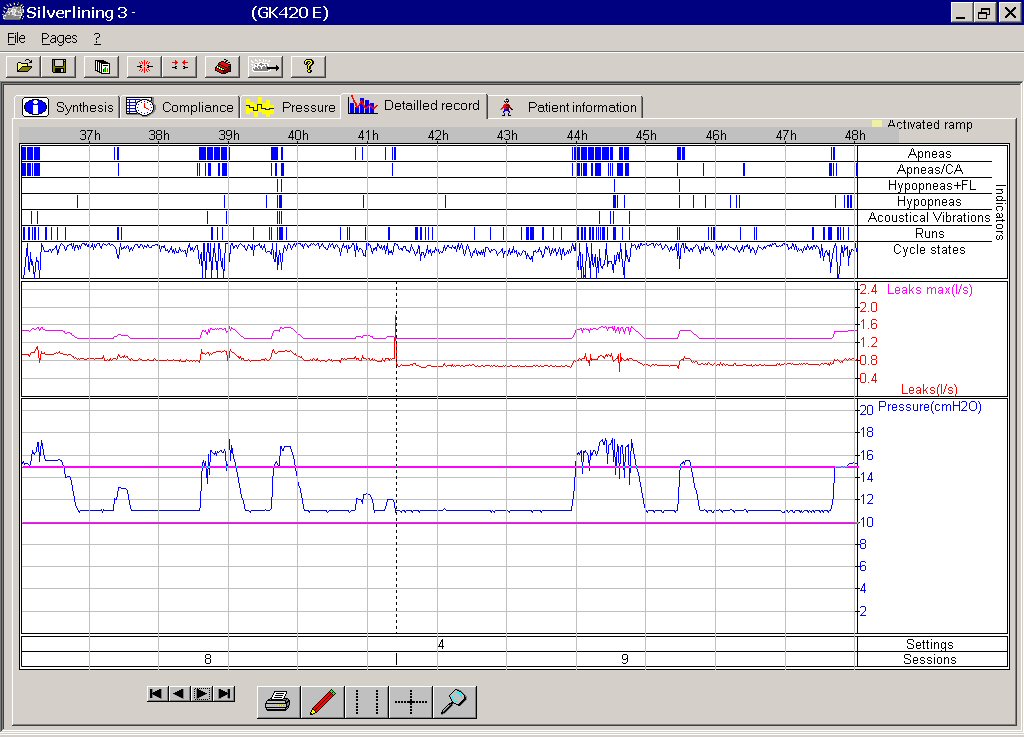
Here's the kind of nights loonlvr was fighting on a regular basis - sudden heavy clusters of events:
Mar 10, 2005 subject: What is the REMStar Auto really doing? starting on page 3 - loonlvr's chart
Looking back through that thread, interestingly, Mikesus mentioned:
"Well another possibility is that he is having an obstruction that is not only non- responsive, but can not be resolved with cpap. (Vocal Cord Disfunction, sleeping on the hose and crushing it?)" (emphasis mine) WTG, Mikesus!
Mar 18, 2005 subject: What's REMStar Auto Really Doing? - new thread using autopap in cpap mode - loonlvr's chart
Loonlvr still got heavy clusters after switching to the 420E Autopap:
loonlvr-before-No_Prilosec_or_Benadryl.jpg
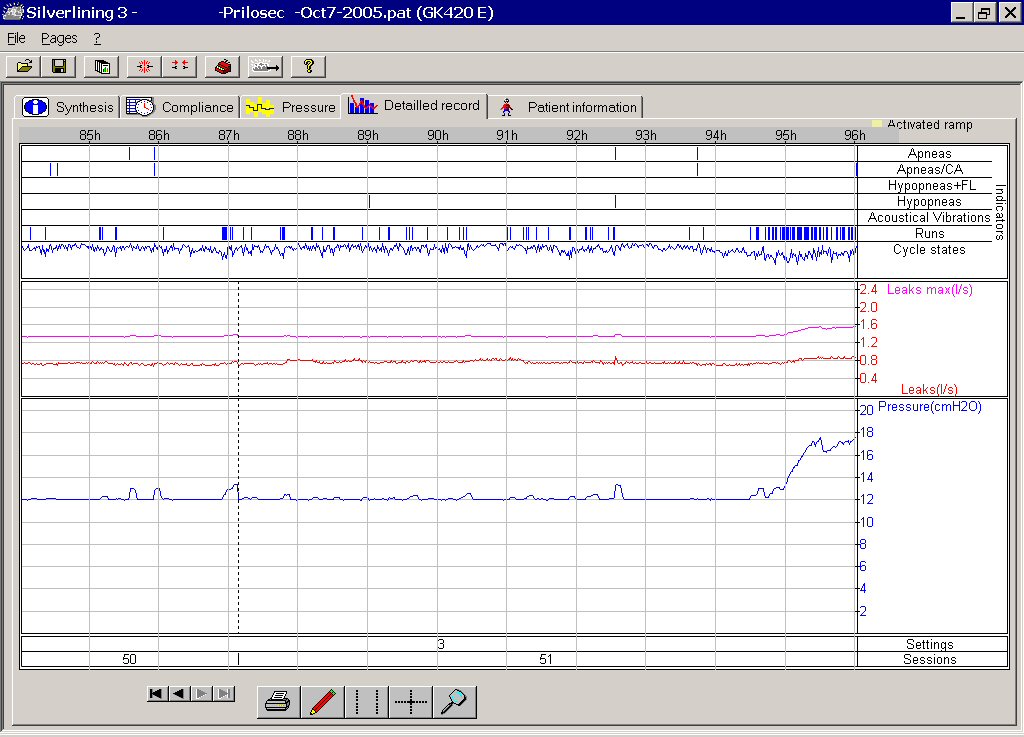
After several days on Prilosec and Benadryl, loonlvr started getting wonderful consistent results like this:
loonlvr-after-With_Prilosec_and_Benadryl.jpg
It's very possible that with Prilosec now preventing the throat and/or vocal cords from being bathed with acid, and the Benadryl reducing tissue swelling in the throat, the REMstar also would give you equally good results, loonlvr. Might not be that one machine responds faster at all.
My next post below contains -SWS's thoughts back when he was working on loonlvr's problem.
Very, very happy for you!! Thanks for posting about what you did. You may be helping any number of people out there who are still struggling with their treatment and have not considered undiagnosed or "silent" acid reflux. Many have reported that CPAP treatment cleared up their GERD symptoms. But for others GERD apparently can interfere with getting good CPAP treatment at all.
Here's the kind of nights loonlvr was fighting on a regular basis - sudden heavy clusters of events:
Mar 10, 2005 subject: What is the REMStar Auto really doing? starting on page 3 - loonlvr's chart
Looking back through that thread, interestingly, Mikesus mentioned:
"Well another possibility is that he is having an obstruction that is not only non- responsive, but can not be resolved with cpap. (Vocal Cord Disfunction, sleeping on the hose and crushing it?)" (emphasis mine) WTG, Mikesus!
Mar 18, 2005 subject: What's REMStar Auto Really Doing? - new thread using autopap in cpap mode - loonlvr's chart
Loonlvr still got heavy clusters after switching to the 420E Autopap:
loonlvr-before-No_Prilosec_or_Benadryl.jpg
{kind=link}
After several days on Prilosec and Benadryl, loonlvr started getting wonderful consistent results like this:
loonlvr-after-With_Prilosec_and_Benadryl.jpg
{kind=link}
It's very possible that with Prilosec now preventing the throat and/or vocal cords from being bathed with acid, and the Benadryl reducing tissue swelling in the throat, the REMstar also would give you equally good results, loonlvr. Might not be that one machine responds faster at all.
My next post below contains -SWS's thoughts back when he was working on loonlvr's problem.
Last edited by rested gal on Sun Nov 06, 2005 2:35 am, edited 4 times in total.
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
From -SWS, regarding loonlvr's data and cluster problem:
Laura, the Remstar and PB data tell the same SDB story,
but each with a separate spin. The RemStar Auto does not
explicitly distinguish central apneas. Rather the Remstar
distinguishes those apneas that do not resolve after three
pressure increments as "non responsive" apneas. Apneas that
happen to go away within those three pressure increments
are categorized as "obstructive apneas". In the Remstar's
case some of those apneas that default into this later
"obstructive apnea" category are actually central in nature.
The PB detection and scoring method distinguishes
(central-versus-obstructive apneas) much better via detection
of cardiac oscillations. In addition the Remstar tends
to refrain from delivering therapeutic pressure once a
non-responsive apnea has been encountered.
By contrast the 420e will attempt to distinguish central
versus obstructive apneas and treat obstructive apneas
accordingly. In the course of algorithmically making this
crucial distinction the 420e treats Mike marginally better.
The 420e also bears out that these "strings" or "densely
packed clusters" of apneas can be predominately central for
Mike. Neither AutoPAP algorithm treats Mike exceptionally
well, however.
The question unanswered by both data sets is: Why does Mike
experience these somewhat atypical clusters of apneas in the
first place? Several possibilities come to mind and I will
list them in order of what I **think** the likelihood may be:
1) Central Apneas Driven By "Positive Pressure Slopes"
or "Pressure Increases": You may recall in a prior
email that I had mentioned central apneas tend not to induce
so much by fixed pressure as they tend to induce by increasing
pressure. Sleep technicians titrating a fixed pressure often
find that they must increase pressure very slowly to avoid
inducing central apneas in some patients. These patients
in particular may actually fare better at a fixed pressure,
or at least with a very narrow AutoPAP pressure range that
restricts upward pressure swings. The 420e in particular
can be set to increase pressure in either 1 cm increments
or .5 cm increments. This type of patient would likely fare
better with the lesser .5 cm pressure increments.
However, these "pressure slope sensitive" patients may fare
even better at fixed pressure than dynamically varying
pressures. I for one would be very interested in seeing
Mike's AHI while running at 11 cm fixed pressure, and I
would be very interested in seeing his AHI at 12 cm fixed
pressure as well. These fixed pressure experiments in
particular could bear out whether Mike's "strings" of apneas
are, indeed, induced by the positive pressure slopes
AutoPAPs deliver throughout the night.
2) Respiratory Swelling or Airway Constriction:
This is an airway obstruction that is autoimmune and/or
vascular based rather than the typical apneic obstruction
involving the upper airway dilator muscles. These tend
not to be easily resolved by air pressure therapy. You
might recall old TAS posts in which Royler and Jerryreb
both discovered their SDB would only resolve when they
happen to be on prednisone. Unfortunately the long-term
effects of prednisone are far worse than a few unresolved
nightly apneas. Neither of these two posters ever found
a way to completely resolve their outstanding SDB events
with air pressure therapy alone.
A doctor-supervised short-term experiment with prednisone
may bear out the true nature of Mike's unresolved apneas
and hypopneas. Alternately over-the-counter Benadryl
may or may not help Mike at night. (emphasis mine)
3) Body Position: Depending on unique thoracic
and/or pharyngeal characteristics, some patients may
actually develop airway obstructions throughout the night
based on body position. If I turn my own head sharply to
the right or left, for instance, I encounter significantly
more airway resistance. If I were to do this in my sleep,
I might experience those hypopneas of mine which tend
not to easily resolve with air pressure.
An intermittently receding mandible would be another
example of an episodic yet persistent airway obstruction
that would not easily resolve with air pressure alone
in some patients. A video recording with a visual time
reference might be used toward correlating unresolved
apneas/hypopneas with body position. A boil-and-bite
mouth guard used in conjunction with a firm chin strap
might experimentally confirm (albeit only partially
alleviate) a mandible that intermittently recedes and
obstructs throughout the night.
4) Combinational Issues: We always want to find "the"
solution, even when working on highly complex problems.
Complex problems in particular can be multifactorial in
nature. Or stating it more simply: Sometimes there are
several contributing factors. Any combination of the
above might come into play for Mike, or any combination
of factors not even mentioned above may really be at the
heart of Mike's unresolved apneas.
Hope this helps at least a bit, Laura.
____________________________________________________
Then, HERE's where –SWS almost certainly nailed loonlvr's
problem and the solution:
Sun, 11 Sep 2005 09:52:16 -0500
Laura, I thought of another possibility to throw into
the mix after I sent you that email. Namely, vocal chord
spasms. Researchers believe that at least some apneas
and hypopneas may not involve the upper dilator muscles---
but rather are a function of the vocal chords themselves
experiencing spasms. Those who subscribe to this school
of thought attribute these vocal chord spasms to repeated
or ongoing exposure to stomach acid (among other possible
causes or physiological triggers such as stress).
Looking at Mike's (somewhat atypical) "strings" or
clusters of SDB events I can't help but wonder if this
vocal-chord-based etiology doesn't fit his particular
pattern of events:
1) isolated episodes, as are typical of spasms in general.
2) unrelated to sleep stage, unlike typical upper airway
dilator muscle apneas. (Mike can have one-to-two hour
episodes, which outlast several sleep stages.)
3) long strings of mixed events are sometimes shown on
Mike's SL3 reports---meaning sometimes his airway is
open enough to convey cardiac oscillations (as an
inefficient acoustical waveguide) and yet other times
there are no cardiac oscillations present (sometimes
there are even interspersed snores).
I think the above pattern just might fit episodes of
vocal chord spasms.
If so, a visit to an upper GI specialist for evaluation
of possible acid reflux disease (GERD or even LPR) might
be in order. Short of a doctor's visit one possible
experiment might be to incorporate those same lifestyle
changes that people with acid reflux disease typically
implement:
1) dietary changes---
minimizing acidic foods and beverages as well as restricting
consumption late in the day/evening
2) sleep with head slightly elevated
3) over-the-counter or prescription medication to either
neutralize or minimize production of stomach acids.
(emphasis mine)
Laura, the Remstar and PB data tell the same SDB story,
but each with a separate spin. The RemStar Auto does not
explicitly distinguish central apneas. Rather the Remstar
distinguishes those apneas that do not resolve after three
pressure increments as "non responsive" apneas. Apneas that
happen to go away within those three pressure increments
are categorized as "obstructive apneas". In the Remstar's
case some of those apneas that default into this later
"obstructive apnea" category are actually central in nature.
The PB detection and scoring method distinguishes
(central-versus-obstructive apneas) much better via detection
of cardiac oscillations. In addition the Remstar tends
to refrain from delivering therapeutic pressure once a
non-responsive apnea has been encountered.
By contrast the 420e will attempt to distinguish central
versus obstructive apneas and treat obstructive apneas
accordingly. In the course of algorithmically making this
crucial distinction the 420e treats Mike marginally better.
The 420e also bears out that these "strings" or "densely
packed clusters" of apneas can be predominately central for
Mike. Neither AutoPAP algorithm treats Mike exceptionally
well, however.
The question unanswered by both data sets is: Why does Mike
experience these somewhat atypical clusters of apneas in the
first place? Several possibilities come to mind and I will
list them in order of what I **think** the likelihood may be:
1) Central Apneas Driven By "Positive Pressure Slopes"
or "Pressure Increases": You may recall in a prior
email that I had mentioned central apneas tend not to induce
so much by fixed pressure as they tend to induce by increasing
pressure. Sleep technicians titrating a fixed pressure often
find that they must increase pressure very slowly to avoid
inducing central apneas in some patients. These patients
in particular may actually fare better at a fixed pressure,
or at least with a very narrow AutoPAP pressure range that
restricts upward pressure swings. The 420e in particular
can be set to increase pressure in either 1 cm increments
or .5 cm increments. This type of patient would likely fare
better with the lesser .5 cm pressure increments.
However, these "pressure slope sensitive" patients may fare
even better at fixed pressure than dynamically varying
pressures. I for one would be very interested in seeing
Mike's AHI while running at 11 cm fixed pressure, and I
would be very interested in seeing his AHI at 12 cm fixed
pressure as well. These fixed pressure experiments in
particular could bear out whether Mike's "strings" of apneas
are, indeed, induced by the positive pressure slopes
AutoPAPs deliver throughout the night.
2) Respiratory Swelling or Airway Constriction:
This is an airway obstruction that is autoimmune and/or
vascular based rather than the typical apneic obstruction
involving the upper airway dilator muscles. These tend
not to be easily resolved by air pressure therapy. You
might recall old TAS posts in which Royler and Jerryreb
both discovered their SDB would only resolve when they
happen to be on prednisone. Unfortunately the long-term
effects of prednisone are far worse than a few unresolved
nightly apneas. Neither of these two posters ever found
a way to completely resolve their outstanding SDB events
with air pressure therapy alone.
A doctor-supervised short-term experiment with prednisone
may bear out the true nature of Mike's unresolved apneas
and hypopneas. Alternately over-the-counter Benadryl
may or may not help Mike at night. (emphasis mine)
3) Body Position: Depending on unique thoracic
and/or pharyngeal characteristics, some patients may
actually develop airway obstructions throughout the night
based on body position. If I turn my own head sharply to
the right or left, for instance, I encounter significantly
more airway resistance. If I were to do this in my sleep,
I might experience those hypopneas of mine which tend
not to easily resolve with air pressure.
An intermittently receding mandible would be another
example of an episodic yet persistent airway obstruction
that would not easily resolve with air pressure alone
in some patients. A video recording with a visual time
reference might be used toward correlating unresolved
apneas/hypopneas with body position. A boil-and-bite
mouth guard used in conjunction with a firm chin strap
might experimentally confirm (albeit only partially
alleviate) a mandible that intermittently recedes and
obstructs throughout the night.
4) Combinational Issues: We always want to find "the"
solution, even when working on highly complex problems.
Complex problems in particular can be multifactorial in
nature. Or stating it more simply: Sometimes there are
several contributing factors. Any combination of the
above might come into play for Mike, or any combination
of factors not even mentioned above may really be at the
heart of Mike's unresolved apneas.
Hope this helps at least a bit, Laura.
____________________________________________________
Then, HERE's where –SWS almost certainly nailed loonlvr's
problem and the solution:
Sun, 11 Sep 2005 09:52:16 -0500
Laura, I thought of another possibility to throw into
the mix after I sent you that email. Namely, vocal chord
spasms. Researchers believe that at least some apneas
and hypopneas may not involve the upper dilator muscles---
but rather are a function of the vocal chords themselves
experiencing spasms. Those who subscribe to this school
of thought attribute these vocal chord spasms to repeated
or ongoing exposure to stomach acid (among other possible
causes or physiological triggers such as stress).
Looking at Mike's (somewhat atypical) "strings" or
clusters of SDB events I can't help but wonder if this
vocal-chord-based etiology doesn't fit his particular
pattern of events:
1) isolated episodes, as are typical of spasms in general.
2) unrelated to sleep stage, unlike typical upper airway
dilator muscle apneas. (Mike can have one-to-two hour
episodes, which outlast several sleep stages.)
3) long strings of mixed events are sometimes shown on
Mike's SL3 reports---meaning sometimes his airway is
open enough to convey cardiac oscillations (as an
inefficient acoustical waveguide) and yet other times
there are no cardiac oscillations present (sometimes
there are even interspersed snores).
I think the above pattern just might fit episodes of
vocal chord spasms.
If so, a visit to an upper GI specialist for evaluation
of possible acid reflux disease (GERD or even LPR) might
be in order. Short of a doctor's visit one possible
experiment might be to incorporate those same lifestyle
changes that people with acid reflux disease typically
implement:
1) dietary changes---
minimizing acidic foods and beverages as well as restricting
consumption late in the day/evening
2) sleep with head slightly elevated
3) over-the-counter or prescription medication to either
neutralize or minimize production of stomach acids.
(emphasis mine)
That is great that you got resolution to it! It is quite possible that the acid was coming up, irritating your vocal cords and they spasm. If the spasm is long enough, then you will actually have symptoms of Asthma. I would add that besides the above suggestions, you might want to a) get an over night pulse oximetry done, and if the oximetry is still showing desats then b) get evaluated for VCD and possibly asthma. Is is possible that your lungs might have been scarred from the acid. (I am in that group unfortunately) The evaluation would require scoping your cords while they try to cause VCD. I had this done in Denver at National Jewish Research, and it at least will verify that diagnosis. Sometimes getting rid of the irritant will resolve it, sometimes it won't. If it doesn't, you will need to find a speech therapist that is familiar with VCD. Treatment involves a number of breathing techniques that try to force the cords open when they are spasming.
Additionally, getting the gerd treated successfully is extremely important! There are a lot of cases where the medications alone will not resolve the acid and surgical intervention is required. Waiting to get it taken care of will put you at risk for barretts esophagus, a pre-cancerous condition. (the cells of the espohagus actually change)
Kudos to SWS for figuring this out!
Additionally, getting the gerd treated successfully is extremely important! There are a lot of cases where the medications alone will not resolve the acid and surgical intervention is required. Waiting to get it taken care of will put you at risk for barretts esophagus, a pre-cancerous condition. (the cells of the espohagus actually change)
Kudos to SWS for figuring this out!
And now the relatively new people know why we miss -SWS so much.....
Thanks for letting us into the detection process.
I'm very ha[[y for you, loonlvr (I guess you're a Mike too....)
O.
Thanks for letting us into the detection process.
I'm very ha[[y for you, loonlvr (I guess you're a Mike too....)
O.
_________________
| Mask: AirFit™ P10 Nasal Pillow CPAP Mask with Headgear |
| Additional Comments: Machine: Resmed AirSense10 for Her with Climateline heated hose ; alternating masks. |
2 posts
• Page 1 of 1