OutaSync wrote:I do have GERD (have the head of my bed raised), I often wake up having bitten my cheek or lips...
Perhaps something's going on here that detracts from restful sleep architecture, Bev. That cheek/lip biting could be the result of GERD eruptions, undiagnosed bruxism, or even a defensive response to those unresolved apneas. Then again it could be unrelated to all the above. But I don't think it's indicative of restorative sleep.
OutaSync wrote:I have a lot of back and shoulder pain from a fall two years ago (had surgery in March, somewhat better now)
Pain can and will utterly devastate my sleep architecture. For me it's neuralgia pain. And when that pain acts up even slightly, I'm a slap happy semi-comical walking zombie!
OutaSync wrote:and I don't think I take any medications that might affect my sleep other than Ambien, which is the only reason I can even get to sleep.
If we take the Ambien out of the above statement, what might account for that part I have underlined? Caffeine? Circadian rhythm disorder? Stress? Bad sleep hygiene by definition? Anxiety about poor-quality sleep related to unresolved SDB? Bev, my layperson's hunch is that resolving the part I have underlined just may turn out to be even more important than trying a new machine.
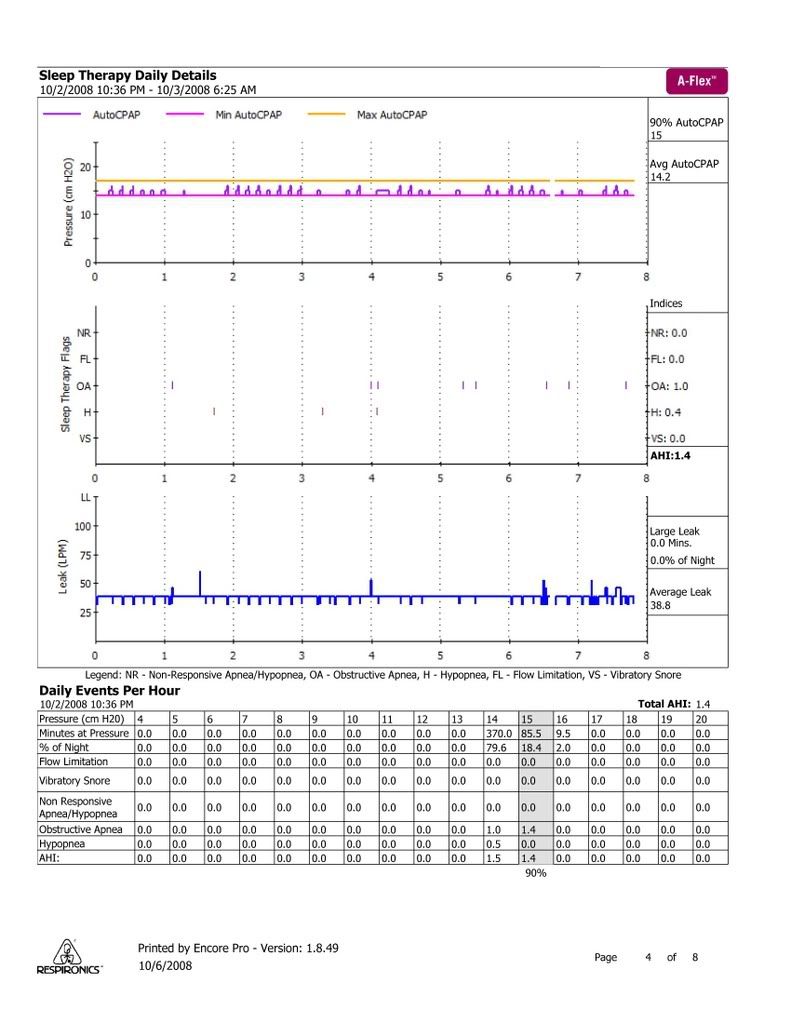
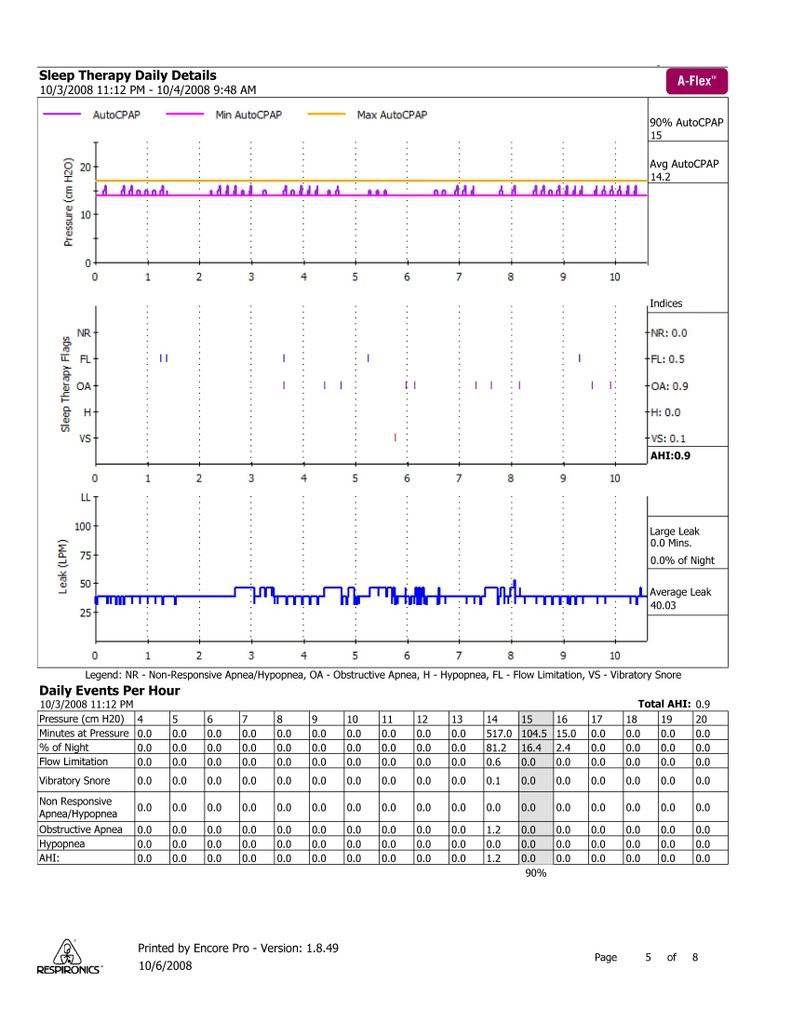
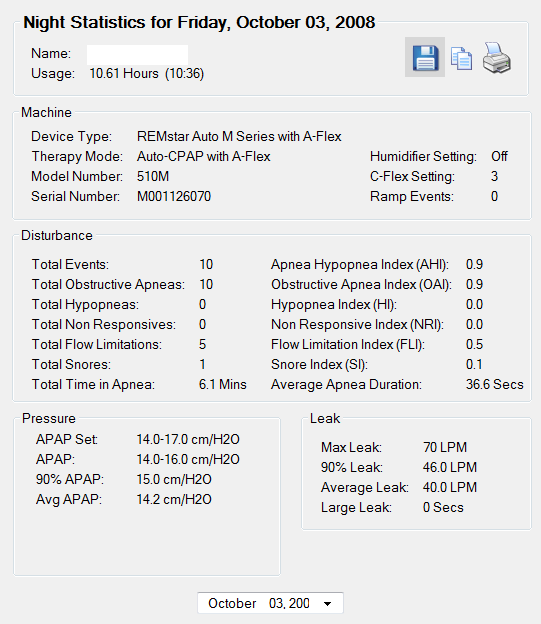
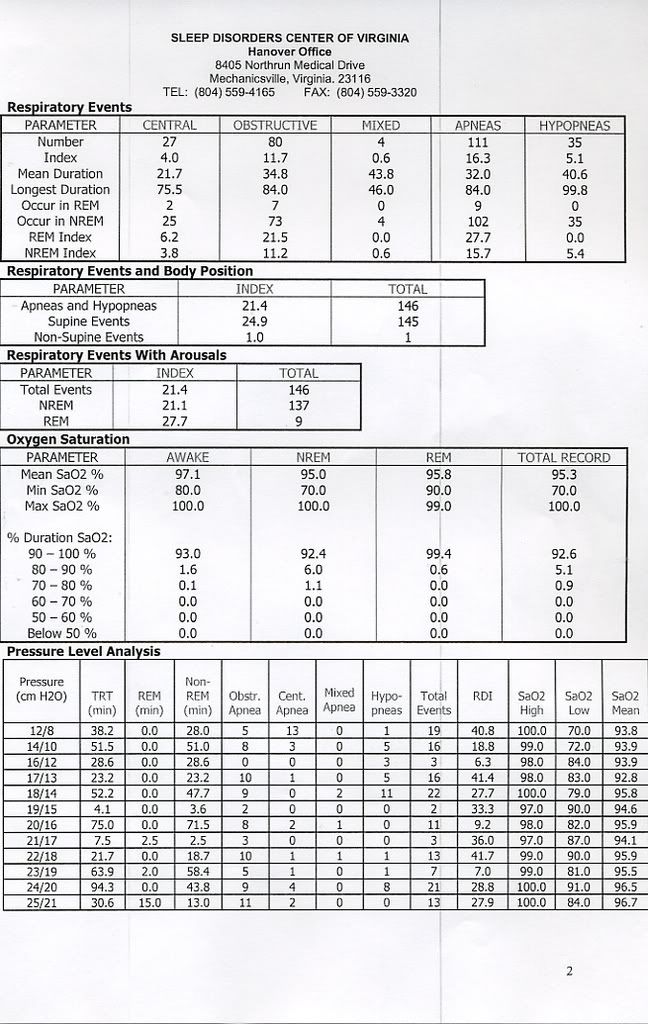
OutaSync wrote:If the APAP missed a few 15 second apneas, I guess that would not be so bad, but if they average 36 seconds, some of them must be longer than that... Is there a machine that would be better for me.
Any algorithm that doesn't take a pass on the first apnea might very well take care of those isolated stragglers. The 420e might be a good algorithm to try. But that's assuming those isolated stragglers are not central, not mixed, or not sympathetic/defensive type closures.
My hunch is that simply fixing those isolated straggler apneas may not sufficiently fix up your sleep problems and daytime energy issues. I have a hunch that you may have a variety of sleep issues that need to be collectively addressed. Perhaps it's time to find a more cooperative sleep doctor.