






Hey Will,
Thanks! I know SWS means well and is providing the most technically accurate decription he knows how. The problem is he "knows how" a lot better than the rest of us.
As I see it the third "command on apnea" is fairly straight forward as described.
The other two as I understand it are such that they are to be left on unless you have one or both of two unique breathing patterns that might fool the machine into unnecessarily reacting. In which case you would want to turn one or both off. The first being "flow limitation runs" IFL1 and the second being "flow limitation with amplitude decrease" IFL2. My understanding as to how you determine if you have one of these is less clear. Maybe SWS can elaborate some more in that regard.
Bman: Spirit Overnight Indices
-
wading thru the muck!

- Posts: 2799
- Joined: Tue Oct 19, 2004 11:42 am
-
WillSucceed

- Posts: 1031
- Joined: Sun Nov 07, 2004 7:52 am
- Location: Toronto, Ontario
Settings
I entirely agree with you -->the problem here is NOT SWS, it is that I don't understand the techno-stuff and jargon.
So, it begs the questions, what, exactly, in simple terms, is a:
1) flow limitation run
2) flow limitation with amplitude decrease.
I'm sorry to flog a dead horse, but I'd bet that I am not the only one that reads the detailed responses, scratches his or her head and says "ok, so what does that mean?" I'm not trying to be cheeky here... I really want to understand this stuff before I bite the bullet and purchase an autopap machine.
P
So, it begs the questions, what, exactly, in simple terms, is a:
1) flow limitation run
2) flow limitation with amplitude decrease.
I'm sorry to flog a dead horse, but I'd bet that I am not the only one that reads the detailed responses, scratches his or her head and says "ok, so what does that mean?" I'm not trying to be cheeky here... I really want to understand this stuff before I bite the bullet and purchase an autopap machine.
P
-
wading thru the muck!
- Posts: 2799
- Joined: Tue Oct 19, 2004 11:42 am
Hi again Will,
I think I can help you there. This is how I understand it.
Central Apnea - air flow stops with no effort to breathe (open airway?)
Obstructive Apnea- air flow stops with effort to breathe (closed airway)
Hypopnea - Amount (amplitude) of air flow decreases (partially closed airway?)
Flow limitation with amplitude decrease IFL2 - Air flow decrease but not to the degree of the hypopnea.
Flow limited run IFL1 - Air flow decrease but not to the degree of IFL2
This is probably over simplified but I think the last three are basically the same thing to varying degrees.
SWS if you can tweek what I've said to make it more accurate (or accurate at all) please do so.
I think I can help you there. This is how I understand it.
Central Apnea - air flow stops with no effort to breathe (open airway?)
Obstructive Apnea- air flow stops with effort to breathe (closed airway)
Hypopnea - Amount (amplitude) of air flow decreases (partially closed airway?)
Flow limitation with amplitude decrease IFL2 - Air flow decrease but not to the degree of the hypopnea.
Flow limited run IFL1 - Air flow decrease but not to the degree of IFL2
This is probably over simplified but I think the last three are basically the same thing to varying degrees.
SWS if you can tweek what I've said to make it more accurate (or accurate at all) please do so.
Sincerely,
wading thru the muck of the sleep study/DME/Insurance money pit!
wading thru the muck of the sleep study/DME/Insurance money pit!
Sorry Guys!
Sorry guys... That is a recurring problem of mine. I do not think "user friendly" as I should. That's a very special skill that Rested Gal and many others who I admire here have, and I wish I had it. As hard as I try, sometimes I fail miserably as I did in the above post. Thank you LDuyer for your ultra-polite way of bringing this to my attention in your PM. I appreciate your kindness.
With that said, let me try another pass at explaining those three parameters.
Command on Apnea: an adjustable parameter to limit just how high the AutoPAP is allowed to go (pressure-wise) in response to any apnea. However, it does not limit how high the AutoPAP is allowed to go in response to all other obstructive sleep event types. This is a safeguard to prevent accidentally causing central apneas with too much air pressure. The reason this pressure safety limit exists for apneas and not other obstructive types such as snore or flow limitation: the 420e cannot always safely distinguish a central apnea from an obstructive apnea (even with "cardiac oscillation detection techniques" that others here have talked about). This command-on-apnea parameter comes factory set at 10 cm since that pressure value is known to be statistically "best" for most people. However, some patients might still have central apneas with this setting. Their central apneas may or may not be because this 10 cm is not a low enough "protection limit" for them. For these patients the command-on-apnea setting should be cautiously and experimentally lowered to see if the central apneas go away and if the obstructions are still being treated adequately. These patients may actually need a BiLevel that is better suited to treat central apneas rather than simply trying to avoid causing too many central apneas with high pressures.
The other reason to change that 10 cm default setting would be patients that have "heavier" than usual obstructions. The 420e will try to prevent as many apneas as possible with a "smart" delivery of air pressure. The 420e will not limit itself to 10 cm as it prevents any sleep events, apneas included. However, as hard as it trys, the 420e must also "respond" to apneas. That responsive scenario is what the "command on apnea" parameter is trying to limit (pressure-wise). So this second reason to change the "command on apnea" 10 cm limit has to do with patients that not only need plenty of "responsive" pressure treatment (versus "proactive" pressure treatment)----but the fact that these unusual patients also need more that 10 cm pressure to clear their obstructive apneas. For these patients, the command-on-apnea would be experimentally raised. The therapist would hope to see that they have fewer obstructive apneas, but not at the expense of pressure-inducing central apneas at those higher pressure.
Before going on to the IFL parameters, let's take a break for some feedback. How is this level of detail? Are there areas that need clarification? I REALLY wish I had Rested Gal's communication skills about now...
I must say, however, the reason nobody here or on the other message boards don't seem to understand this topic is because it is fairly complex. When I hear someone ask me for a quick and simple explanation of precisely what sleep therapists struggle with, it really reminds me of someone jumping into the cockpit of a 747 and saying: "Quick!!! Teach me how to fly this thing... and please make it simple!!!"
With that said, let me try another pass at explaining those three parameters.
Command on Apnea: an adjustable parameter to limit just how high the AutoPAP is allowed to go (pressure-wise) in response to any apnea. However, it does not limit how high the AutoPAP is allowed to go in response to all other obstructive sleep event types. This is a safeguard to prevent accidentally causing central apneas with too much air pressure. The reason this pressure safety limit exists for apneas and not other obstructive types such as snore or flow limitation: the 420e cannot always safely distinguish a central apnea from an obstructive apnea (even with "cardiac oscillation detection techniques" that others here have talked about). This command-on-apnea parameter comes factory set at 10 cm since that pressure value is known to be statistically "best" for most people. However, some patients might still have central apneas with this setting. Their central apneas may or may not be because this 10 cm is not a low enough "protection limit" for them. For these patients the command-on-apnea setting should be cautiously and experimentally lowered to see if the central apneas go away and if the obstructions are still being treated adequately. These patients may actually need a BiLevel that is better suited to treat central apneas rather than simply trying to avoid causing too many central apneas with high pressures.
The other reason to change that 10 cm default setting would be patients that have "heavier" than usual obstructions. The 420e will try to prevent as many apneas as possible with a "smart" delivery of air pressure. The 420e will not limit itself to 10 cm as it prevents any sleep events, apneas included. However, as hard as it trys, the 420e must also "respond" to apneas. That responsive scenario is what the "command on apnea" parameter is trying to limit (pressure-wise). So this second reason to change the "command on apnea" 10 cm limit has to do with patients that not only need plenty of "responsive" pressure treatment (versus "proactive" pressure treatment)----but the fact that these unusual patients also need more that 10 cm pressure to clear their obstructive apneas. For these patients, the command-on-apnea would be experimentally raised. The therapist would hope to see that they have fewer obstructive apneas, but not at the expense of pressure-inducing central apneas at those higher pressure.
Before going on to the IFL parameters, let's take a break for some feedback. How is this level of detail? Are there areas that need clarification? I REALLY wish I had Rested Gal's communication skills about now...
I must say, however, the reason nobody here or on the other message boards don't seem to understand this topic is because it is fairly complex. When I hear someone ask me for a quick and simple explanation of precisely what sleep therapists struggle with, it really reminds me of someone jumping into the cockpit of a 747 and saying: "Quick!!! Teach me how to fly this thing... and please make it simple!!!"
-
rested gal

- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
IFL1 "on" - the machine checks for situations where the person is not getting enough air flow in and out.
IFL2 "on" - the machine checks for the same thing, but won't take action unless it also sees an "amplitude decrease" in the breathing pattern.
If I've stated those things wrong, please correct it, SWS.
WillSucceed, speaking only about my situation - my normal breathing pattern is apparently so shallow that the 420E's IFL1 trigger was being fooled into thinking that such shallow breaths meant: "her throat must be starting to close, because she's not got enough air flowing in/out - she needs more pressure to open the throat."
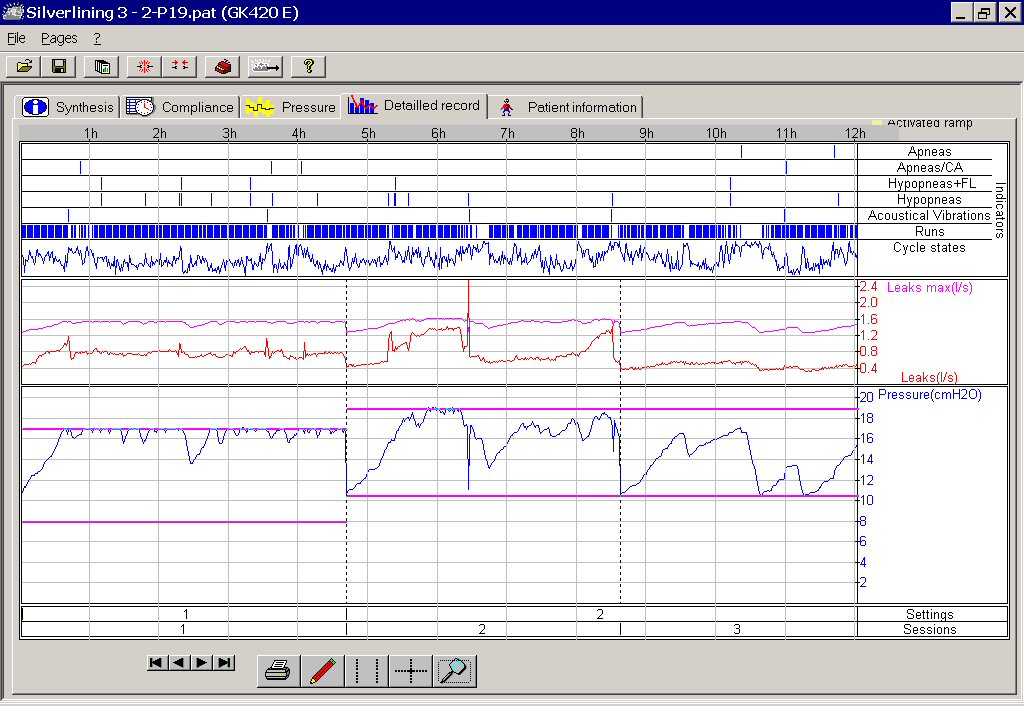
Click the link below to see a picture of my graph with IFL1 and IFL2 both left "on" by default. You'll see where the machine was going bonkers running the pressure up, trying it's best to figure out how to open my throat (which was already open fine.) The session on the left side of this picture was with pressure range set for 8-17. (The pink horizontal lines show the top and bottom of the pressure range I had it set to use.) For the session on the right side of the picture (a new night) I had changed the pressure range to 10 - 19. You can see how wildly the pressure was going up and down trying to find a pressure that would handle what it thought was going on with my "limited flow" breathing. The machine ran up to 18 and 19 a lot.
My difficulty with IFL1 on
I will say... that experience of inhaling/exhaling against pressures of 17, 18 and 19 gave me great emphathy for the people who suffer aerophagia (bloating from swallowed air.) That is painful stuff!
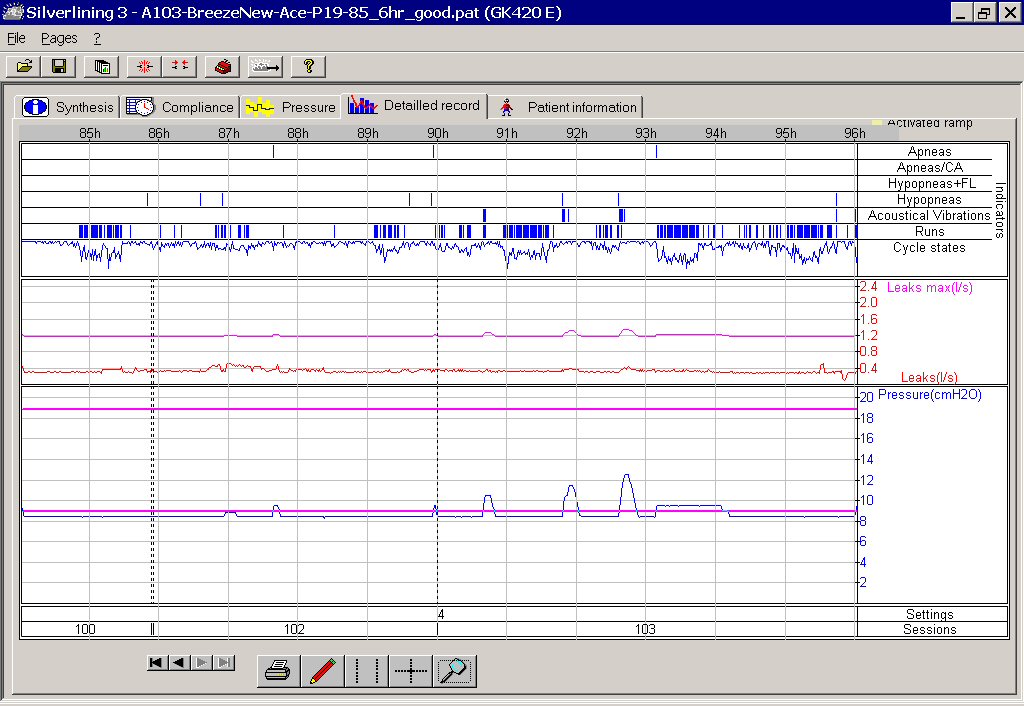
Compare that with the next screenshot, after SWS looked at my graphs and suggested I turn IFL1 OFF... leaving only IFL2 "on". In this picture, the pressure range was still set to allow a top of 19, but now the machine behaved beautifully, easily interpreting my shallow breathing and no longer futilely running the pressure up to the top. The pressure stayed down on 9 most of the two and a half nights shown in the graph. The pressure went up a bit from time to time to deal with things, just like it's supposed to, but it never had to go above 11 and 12 on two occasions. Nothing like the 17, 18, 19 it was wildly running up to when IFL1 was "on".
No problem with IFL1 turned "off", IFL2 left "on"
For most people using the 420E, the defaults of IFL1 "on" and IFL2 'on" can be left as they are - no problem. I hasten to say that, before 420E users think, "OMG, maybe I should turn off IFL1!!!" For me, IFL1 "on" didn't work well, but it would be fine for most.
IFL1 "off", IFL2 "on" - that was the right combo of advanced triggers for me. Perhaps my particular breathing pattern is a rare oddity for the 420E to have to try to deal with. My "shallow breathing" may not have even been the only factor that was confusing the machine. Other shallow breathers probably have no trouble at all with both IFL's left "on". Maybe there's something else about my particular breathing pattern that threw a cog in the wheel and confused the machine in my case
Interestingly, later I got a second machine (got a good deal, so privately bought a 2nd machine for a back-up.) I had quite a bit of trepidation about trying the second machine, as it was not a 420E, which was now behaving so perfectly. The second machine was a REMstar auto. I wondered if the REMstar would also misinterpret my breathing pattern and take off up into the stratosphere...in which case I'd be out of luck, because the REMstar has no separate controls for IFL1, IFL2, etc. So, I cautiously set the upper limit of the REMstar at 16, "just in case", for my first night trying it. Happily, the REMstar handled my breathing pattern fine and behaved itself, never going up anywhere close to 16.
I get equally good treatment with either machine. But, think about this for a moment. What if I had not had the software to see what was happening? Or knowledgeable posters on the message boards, to turn to for advice? I'd have figured, "Well, gee, it sure does take a high pressure for me." Or perhaps I'd have even thought, "Autopaps must not be the kind of machine I should have." Sound like what a doctor who is against autopaps in general might say? heheh
Do I think a doctor, even a "sleep" doctor, could have looked at my initial graphs and figured out what was going on with me and my 420E, much less known what to do about it? I seriously doubt it. Most doctors are not a bit interested in the nuts and bolts of these machines. I credit every bit of good treatment I've enjoyed to the experienced people posting on the message boards.
IFL2 "on" - the machine checks for the same thing, but won't take action unless it also sees an "amplitude decrease" in the breathing pattern.
If I've stated those things wrong, please correct it, SWS.
WillSucceed, speaking only about my situation - my normal breathing pattern is apparently so shallow that the 420E's IFL1 trigger was being fooled into thinking that such shallow breaths meant: "her throat must be starting to close, because she's not got enough air flowing in/out - she needs more pressure to open the throat."
Click the link below to see a picture of my graph with IFL1 and IFL2 both left "on" by default. You'll see where the machine was going bonkers running the pressure up, trying it's best to figure out how to open my throat (which was already open fine.) The session on the left side of this picture was with pressure range set for 8-17. (The pink horizontal lines show the top and bottom of the pressure range I had it set to use.) For the session on the right side of the picture (a new night) I had changed the pressure range to 10 - 19. You can see how wildly the pressure was going up and down trying to find a pressure that would handle what it thought was going on with my "limited flow" breathing. The machine ran up to 18 and 19 a lot.
My difficulty with IFL1 on
{kind=link}
I will say... that experience of inhaling/exhaling against pressures of 17, 18 and 19 gave me great emphathy for the people who suffer aerophagia (bloating from swallowed air.) That is painful stuff!
Compare that with the next screenshot, after SWS looked at my graphs and suggested I turn IFL1 OFF... leaving only IFL2 "on". In this picture, the pressure range was still set to allow a top of 19, but now the machine behaved beautifully, easily interpreting my shallow breathing and no longer futilely running the pressure up to the top. The pressure stayed down on 9 most of the two and a half nights shown in the graph. The pressure went up a bit from time to time to deal with things, just like it's supposed to, but it never had to go above 11 and 12 on two occasions. Nothing like the 17, 18, 19 it was wildly running up to when IFL1 was "on".
No problem with IFL1 turned "off", IFL2 left "on"
{kind=link}
For most people using the 420E, the defaults of IFL1 "on" and IFL2 'on" can be left as they are - no problem. I hasten to say that, before 420E users think, "OMG, maybe I should turn off IFL1!!!" For me, IFL1 "on" didn't work well, but it would be fine for most.
IFL1 "off", IFL2 "on" - that was the right combo of advanced triggers for me. Perhaps my particular breathing pattern is a rare oddity for the 420E to have to try to deal with. My "shallow breathing" may not have even been the only factor that was confusing the machine. Other shallow breathers probably have no trouble at all with both IFL's left "on". Maybe there's something else about my particular breathing pattern that threw a cog in the wheel and confused the machine in my case
Interestingly, later I got a second machine (got a good deal, so privately bought a 2nd machine for a back-up.) I had quite a bit of trepidation about trying the second machine, as it was not a 420E, which was now behaving so perfectly. The second machine was a REMstar auto. I wondered if the REMstar would also misinterpret my breathing pattern and take off up into the stratosphere...in which case I'd be out of luck, because the REMstar has no separate controls for IFL1, IFL2, etc. So, I cautiously set the upper limit of the REMstar at 16, "just in case", for my first night trying it. Happily, the REMstar handled my breathing pattern fine and behaved itself, never going up anywhere close to 16.
I get equally good treatment with either machine. But, think about this for a moment. What if I had not had the software to see what was happening? Or knowledgeable posters on the message boards, to turn to for advice? I'd have figured, "Well, gee, it sure does take a high pressure for me." Or perhaps I'd have even thought, "Autopaps must not be the kind of machine I should have." Sound like what a doctor who is against autopaps in general might say? heheh
Do I think a doctor, even a "sleep" doctor, could have looked at my initial graphs and figured out what was going on with me and my 420E, much less known what to do about it? I seriously doubt it. Most doctors are not a bit interested in the nuts and bolts of these machines. I credit every bit of good treatment I've enjoyed to the experienced people posting on the message boards.
Re: Settings
Thanks, Wader! That helps immensely.
1) snore=slightest airway obstruction and least stifled airway obstruction
2) flow limitation=slightly more stifled or limited patient breathing
3) hypopnea=even more limited airflow than flow limitation
4) apnea=no airflow whatsoever
The medical community also goes into how long the obstruction lasts as part of its criteria regarding which of the above event types an obstruction will be categorized. Absolutely no airflow whatsoever for a very brief moment might be categorized as a hyopnea rather than an apnea. There are subtle differences in how these events are "scored" throughout the international medical community and among manufacturers.
With that said, the above definitions only speak of degrees of airflow and time durations of obstruction. They do not speak of the underlying nature of the airway failure which can often be determined by the very waveform shape of the patient's limited breath. Puritan Bennet and other AutoPAP manufacturers factor in the waveform shape of a patient's limited breath.
So "flow limitation run with amplitude decrease" is a restricted airflow (several breaths actually, hence "F.L. run") that also occurs with hypopneas (hence the "amplitude decrease" part of the name). This would be an example of what are called "concomitant hypopneas". A concomitant hypopnea is a flow limitation and a hypopnea together, which as you can see just doesn't gel with that over-simplified definition above. But, the underlying failing airway mechanism that causes a typical "flow limitation" is not the same airway failure that causes a "hypopnea". They can, indeed, occur simultaneously, and when they do IFL2 will trigger on it because of the unique waveform shape.
A "flow limitation" is a lesser airway restriction that might be caused by nasal or other airway swelling, or perhaps soft pallate partial closure. The air is restricted, but not as severely as with hypopnea or apnea. The 420e requires but several of these limited breaths before it will trigger, hence it is referred to as a "run" or "flow limitation run". Puritan Bennett defines a run as follows: "a Run is detected after two respiratory cycles with flow limitation or ten intermediate respiratory cycles and ends after two successive respiratory cycles without flow limitation.
With that attempt at a layman's explanation, let me list Puritan Bennett's event definitions below:
Apneas:
This refers to respiratory Apnea during which there were no representative cardiac oscillations.
Apneas / CA:
This refers to a respiratory Apnea where representative and permanent cardiac oscillations were detected.
Hypopneas:
This refers to a decrease in the amplitude of breathing.
Hypopneas+FL:
This refers to a RUN of Inspiratory flow limitation with simultaneous reduction in the amplitude of breathing.
Acoustical Vibrations:
This refers to detection of acoustical vibrations caused by the patient snoring.
Runs :
A Run is an indicator of a respiratory period with flow limitation, defined as follows: a Run is detected after two respiratory cycles with flow limitation or ten intermediate respiratory cycles and ends after two successive respiratory cycles without flow limitation.
Cycle status:
The analysis of the flow form during the inspiration computed at each respiratory cycle allows their classification in Normal (N), Intermediate (I) or at Flow Limitation (FL). On the trend trace, the higher the trace, the closer the inspiratory cycles are to normal (N). Conversely, a low trace indicates a trend of Flow Limitation (FL). A median trace indicates a trend of intermediate cycles (I).
Flow limitations, flow limitation runs, and hypopneas are collectively the source of debate within the sleep industry and medical/scientific community in general. The above need to be defined according to Puritan Bennett's criteria, but first I want to give you the over-simplified definition that we patients use, that just so happens to not match what Puritan Bennet means by the above. The over-simplified definition is comprised of how much airflow is occuring in a patient's breath:WillSucceed wrote: 1) flow limitation run
2) flow limitation with amplitude decrease.
1) snore=slightest airway obstruction and least stifled airway obstruction
2) flow limitation=slightly more stifled or limited patient breathing
3) hypopnea=even more limited airflow than flow limitation
4) apnea=no airflow whatsoever
The medical community also goes into how long the obstruction lasts as part of its criteria regarding which of the above event types an obstruction will be categorized. Absolutely no airflow whatsoever for a very brief moment might be categorized as a hyopnea rather than an apnea. There are subtle differences in how these events are "scored" throughout the international medical community and among manufacturers.
With that said, the above definitions only speak of degrees of airflow and time durations of obstruction. They do not speak of the underlying nature of the airway failure which can often be determined by the very waveform shape of the patient's limited breath. Puritan Bennet and other AutoPAP manufacturers factor in the waveform shape of a patient's limited breath.
So "flow limitation run with amplitude decrease" is a restricted airflow (several breaths actually, hence "F.L. run") that also occurs with hypopneas (hence the "amplitude decrease" part of the name). This would be an example of what are called "concomitant hypopneas". A concomitant hypopnea is a flow limitation and a hypopnea together, which as you can see just doesn't gel with that over-simplified definition above. But, the underlying failing airway mechanism that causes a typical "flow limitation" is not the same airway failure that causes a "hypopnea". They can, indeed, occur simultaneously, and when they do IFL2 will trigger on it because of the unique waveform shape.
A "flow limitation" is a lesser airway restriction that might be caused by nasal or other airway swelling, or perhaps soft pallate partial closure. The air is restricted, but not as severely as with hypopnea or apnea. The 420e requires but several of these limited breaths before it will trigger, hence it is referred to as a "run" or "flow limitation run". Puritan Bennett defines a run as follows: "a Run is detected after two respiratory cycles with flow limitation or ten intermediate respiratory cycles and ends after two successive respiratory cycles without flow limitation.
With that attempt at a layman's explanation, let me list Puritan Bennett's event definitions below:
Apneas:
This refers to respiratory Apnea during which there were no representative cardiac oscillations.
Apneas / CA:
This refers to a respiratory Apnea where representative and permanent cardiac oscillations were detected.
Hypopneas:
This refers to a decrease in the amplitude of breathing.
Hypopneas+FL:
This refers to a RUN of Inspiratory flow limitation with simultaneous reduction in the amplitude of breathing.
Acoustical Vibrations:
This refers to detection of acoustical vibrations caused by the patient snoring.
Runs :
A Run is an indicator of a respiratory period with flow limitation, defined as follows: a Run is detected after two respiratory cycles with flow limitation or ten intermediate respiratory cycles and ends after two successive respiratory cycles without flow limitation.
Cycle status:
The analysis of the flow form during the inspiration computed at each respiratory cycle allows their classification in Normal (N), Intermediate (I) or at Flow Limitation (FL). On the trend trace, the higher the trace, the closer the inspiratory cycles are to normal (N). Conversely, a low trace indicates a trend of Flow Limitation (FL). A median trace indicates a trend of intermediate cycles (I).
Last edited by -SWS on Sat Jan 15, 2005 6:29 am, edited 1 time in total.
Nicely Explained...
Thanks, RG! You always do that so well!
IFL1 IFL2
I think that's not a bad way of stating it, Rested Gal. "Amplitude decrease" is a hyponea. So IFL1 will trigger on several "flow limited" breaths. It will, based on that trigger, go off to a separate part of the pressure-response algorithm and deliver the magnitude and duration of pressure that PB thinks best handles that exact breathing scenario.rested gal wrote:IFL1 "on" - the machine checks for situations where the person is not getting enough air flow in and out.
IFL2 "on" - the machine checks for the same thing, but won't take action unless it also sees an "amplitude decrease" in the breathing pattern.
IFL2 will trigger on "flow limited breaths that simultaneously show a hypopnea waveforfm". When IFL2 triggers the 420e will go off to that part of the algorithm and deliver the magnitude and duration of pressure that PB thinks best handles that exact breathing scenario.
However, "shallow breathing" would essentially be an issue of respiratory drive and not obstruction. So "shallow breathing" at night would manifest as central hypopneas---not to be confused with obstructive hypopneas. IFL1 and IFL2 are both actually geared toward UARS type obstructions, which are not thought to be central in nature. However, your shallow breaths could very well have been misinterpreted by IFL1 as obstructive flow limitations, which of course, they were not. The 420e attempts to recognize the difference between non-apneic hypopneas by differentiating wave shape (obstructive events more often being differentiated by eclipsing and/or resonating tissue with a corresponding "obstructive appearing" breath wave shape). That IFL2 trigger, which is really "flow run plus hypopnea" has statistical implications: that concomitant hypopnea has a much less chance of being central in nature than had it occured alone, and therefore more pressure can be safely delivered. Hence the dedicated pressure-response routine in the algorithm when that waveform shape and amplitude is detected.
This is very complicated stuff... I am sorry that I am not a better explainer!
Last edited by -SWS on Sat Jan 15, 2005 6:53 am, edited 1 time in total.
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
SWS, the more you post on technical issues, the better.
Whether I "get it" or not, the first time or ever, the more analytical information you share about the mechanics of this kind of therapy, the better. I especially appreciate your patience, precision and accuracy in re-explaining this tough stuff.
While I don't understand much about complicated technical matters, I do like having such discussions available for me to keep reading over and over.
Even if only one particular sentence within a technical discussion makes a lightbulb go off, or gives a person a glimpse of something to ask their doctor about, that might just be what enables someone and his/her doctor to get started down a better treatment trail.
SWS, keep those techie posts comin', please!
Whether I "get it" or not, the first time or ever, the more analytical information you share about the mechanics of this kind of therapy, the better. I especially appreciate your patience, precision and accuracy in re-explaining this tough stuff.
While I don't understand much about complicated technical matters, I do like having such discussions available for me to keep reading over and over.
Even if only one particular sentence within a technical discussion makes a lightbulb go off, or gives a person a glimpse of something to ask their doctor about, that might just be what enables someone and his/her doctor to get started down a better treatment trail.
SWS, keep those techie posts comin', please!
Rested Gal's graphs
Thanks again, Rested Gal!!! Those two graphs will undoubtedly look "Greek" to many or most people here. For those so inclined to visually sort through all that data, here are a couple noteworthy observations about Rested Gal's "before" and "after" graphs:
1) Specifically look at the horizontal graph on each of those two charts called "Runs". Notice on Rested Gal's "before IFL1 is turned off" chart that there are actually many more flow runs than on her "after IFL1 is turned off" chart. Her higher delivered pressures from IFL1 "over-triggering" actually worsened or aggravated the number of "flow runs" that she experienced!
2) On that "before IFL1 is turned off" chart, you can visually correlate when her "runs" start to cluster in great numbers and her 420e erroneously commences a sustained "pressure hike". Looking at only this chart, this visual correlation is admittedly tough to make out. However, looking at several of her charts, her dense clustering of "runs" really start to visually stand out as a having a definite cause-effect (triggering) relationship relative to her long-term pressure hikes.
After turning IFL1 off, her sleep indices relative to non-flow-limitation events stayed more or less the same. However, her flow runs actually improved a bit. More importantly, she slept and felt at least as well as before, without exposing her respiratory tract to unnecessarily high pressures. Other patients undoubtedly would have experienced a variety of unfortunate "over pressure" side effects such as aerophagia, central apneas, etc. from the "over triggering" of IFL1.
This is really complex stuff! In my opinion IFL1, IFL2, and "command on apnea" are parameters that the vast majority of patients will never understand adequately to treat themselves. Nor should they try to treat themselves when they get in trouble. Nor should patients on any message board try to medically treat other patients on a message board, for that matter. Ideally patients having sleep disorders or even sleep therapy problems should search and search until they find a qualified therpist to get their treatment problems rectified. As I said before, many therapist will actually get totally stumped by IFL1, IFL2, and "command on apnea". That is precisely why I think a well-designed AutoPAP really should be an out-of-the box solution that is algorithmically well-designed and well tested toward automatically correcting obvious treatment "faults".
My opinion is not that the 420e is an excellent AutoPAP because it has IFL1, IFL2, and "command on apnea" adjustable parameters. Rather, my opinion is that the 420e is a superb AutoPAP despite having these features that can get so many patients and therapists into trouble.
To answer Will's question about when you should adjust these parameters: No one should adjust them unless they're absolutely crystal clear about what the adjustable parameter is for (in all its technical/physiological complexity), and what the potential physiological and technical ramifications are of changing that parameter. Most patients will find that these three parameters do not need to be adjusted at all since the 420e is not only customizable for statistically anomalous patients, but it is also a great out-of-the box AutoPAP that will serve the masses of OSA patients quite well. Low-end pressure range will admittedly be the one adjustable parameter that quite a few AutoPAP patients will need to adjust to avoid feeling "starved for air".
New patients really should work through set up issues with a trained therapist. Even "seasoned" patients should contact their therapist when treatment is not going well.
1) Specifically look at the horizontal graph on each of those two charts called "Runs". Notice on Rested Gal's "before IFL1 is turned off" chart that there are actually many more flow runs than on her "after IFL1 is turned off" chart. Her higher delivered pressures from IFL1 "over-triggering" actually worsened or aggravated the number of "flow runs" that she experienced!
2) On that "before IFL1 is turned off" chart, you can visually correlate when her "runs" start to cluster in great numbers and her 420e erroneously commences a sustained "pressure hike". Looking at only this chart, this visual correlation is admittedly tough to make out. However, looking at several of her charts, her dense clustering of "runs" really start to visually stand out as a having a definite cause-effect (triggering) relationship relative to her long-term pressure hikes.
After turning IFL1 off, her sleep indices relative to non-flow-limitation events stayed more or less the same. However, her flow runs actually improved a bit. More importantly, she slept and felt at least as well as before, without exposing her respiratory tract to unnecessarily high pressures. Other patients undoubtedly would have experienced a variety of unfortunate "over pressure" side effects such as aerophagia, central apneas, etc. from the "over triggering" of IFL1.
This is really complex stuff! In my opinion IFL1, IFL2, and "command on apnea" are parameters that the vast majority of patients will never understand adequately to treat themselves. Nor should they try to treat themselves when they get in trouble. Nor should patients on any message board try to medically treat other patients on a message board, for that matter. Ideally patients having sleep disorders or even sleep therapy problems should search and search until they find a qualified therpist to get their treatment problems rectified. As I said before, many therapist will actually get totally stumped by IFL1, IFL2, and "command on apnea". That is precisely why I think a well-designed AutoPAP really should be an out-of-the box solution that is algorithmically well-designed and well tested toward automatically correcting obvious treatment "faults".
My opinion is not that the 420e is an excellent AutoPAP because it has IFL1, IFL2, and "command on apnea" adjustable parameters. Rather, my opinion is that the 420e is a superb AutoPAP despite having these features that can get so many patients and therapists into trouble.
To answer Will's question about when you should adjust these parameters: No one should adjust them unless they're absolutely crystal clear about what the adjustable parameter is for (in all its technical/physiological complexity), and what the potential physiological and technical ramifications are of changing that parameter. Most patients will find that these three parameters do not need to be adjusted at all since the 420e is not only customizable for statistically anomalous patients, but it is also a great out-of-the box AutoPAP that will serve the masses of OSA patients quite well. Low-end pressure range will admittedly be the one adjustable parameter that quite a few AutoPAP patients will need to adjust to avoid feeling "starved for air".
New patients really should work through set up issues with a trained therapist. Even "seasoned" patients should contact their therapist when treatment is not going well.
-
rested gal
- Posts: 12880
- Joined: Thu Sep 09, 2004 10:14 pm
- Location: Tennessee
-
wading thru the muck!
- Posts: 2799
- Joined: Tue Oct 19, 2004 11:42 am
Long Disclaimer
Wader, you assuming devil you... You certainly predicted my ensuing "long disclaimer" from a mile away, so here it is:wading thru the muck! wrote:Oh rested gal,
Now we must brace ourselves for a long "disclaimer" by SWS.
D____I____S_____C____L____A____I_____M_____E_____R
Rested Gal, my friend... I certainly owe you one!
Re: Spirit, 420e, etc.
Thanks. This makes sense. When I've used neo-synephrine to keep my nasal passages open, the pressure has dropped quite a bit. Due to the warnings on the bottle, I don't want to use this too often.-SWS wrote:The Spirit is very proactively pressure-agressive regarding flow limitations (as likely precursors to both hypopneic and apneic events). Likely your swollen nasal passages (which are, after all, flow limitations) are trigerring the Spirit to sustain high pressure.
I will probably have a procedure soon using radio waves to shrink my turbinate tissues. It looks like that should improve my nasal situation quite a bit.
I'm happy with the Vista. I've just learned that my problems are probably not mask related. I've had the same problems with the Activa. My doc says I have small nasal passages and enlarged turbinates. I will soon have a procedure using radio waves to shrink those.wading thru the muck! wrote:Are you able to use the Vista without leaks? I have not heard good things about the Vista. If you have large leaks that may also be causing some of the problems you've encountered.
Sounds like when you can keep the mask on you've been doing well.
The Vista leaks more than the Activa, but I tend to push it a little into the pillow. That takes care of the leak and lets me get to sleep. I don't care after I get to sleep. Leaks don't wake me up. After two months the cushion seems to be losing some of its elasticity. I have another on order.
The problem with the Activa is that it is larger and touches more of my face. It's also more snug around the nose. This makes my nose itch. That's more annoying to me than leaks.
I read out the machine every morning and the leaks are within the machines range, so I don't think that's causing problems. The lowest leak I ever see is 0.42L/sec. I assume this is how much escapes out the exhaust vents. On a bad day, it registers a leak of 0.54L/sec, so I guess the leak is not that bad compared with normal mask exhaust.