IFL1 "on" - the machine checks for situations where the person is not getting enough air flow in and out.
IFL2 "on" - the machine checks for the same thing, but won't take action unless it
also sees an "amplitude decrease" in the breathing pattern.
If I've stated those things wrong, please correct it, SWS.
WillSucceed, speaking only about my situation - my normal breathing pattern is apparently
so shallow that the 420E's IFL1 trigger was being fooled into thinking that such shallow breaths meant: "her throat must be starting to close, because she's not got enough air flowing in/out - she needs more pressure to open the throat."
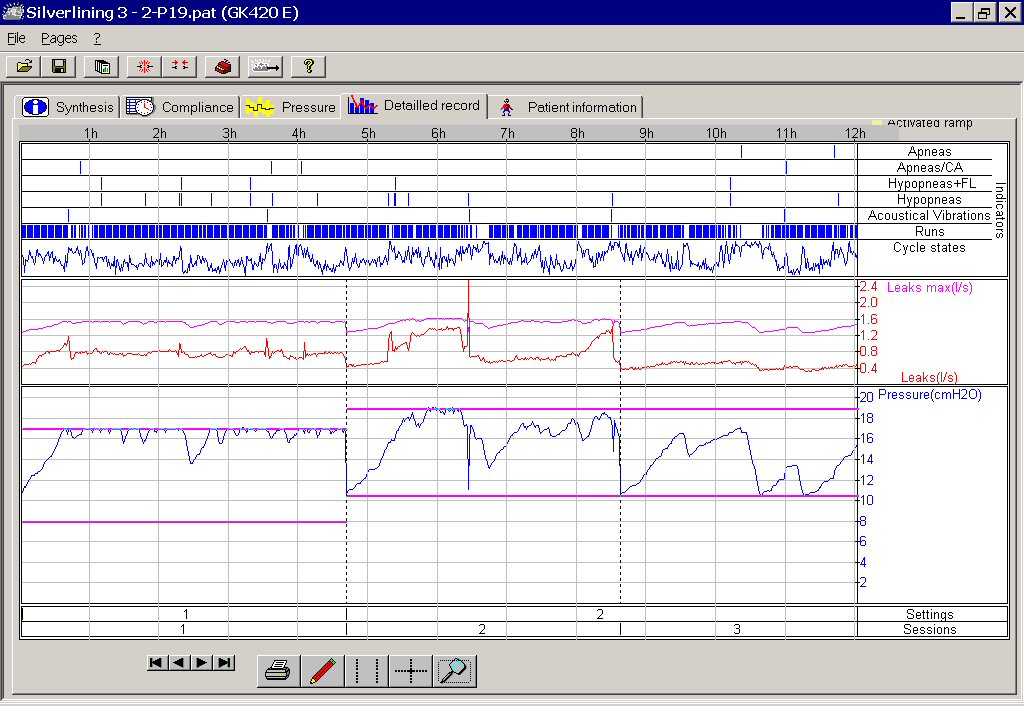
Click the link below to see a picture of my graph with IFL1 and IFL2 both left "on" by default. You'll see where the machine was going bonkers running the pressure up, trying it's best to figure out how to open my throat (which was already open fine.) The session on the left side of this picture was with pressure range set for 8-17. (The pink horizontal lines show the top and bottom of the pressure range I had it set to use.) For the session on the right side of the picture (a new night) I had changed the pressure range to 10 - 19. You can see how wildly the pressure was going up and down trying to find a pressure that would handle what it thought was going on with my "limited flow" breathing. The machine ran up to 18 and 19 a lot.
My difficulty with IFL1 on
I will say... that experience of inhaling/exhaling against pressures of 17, 18 and 19 gave me
great emphathy for the people who suffer aerophagia (bloating from swallowed air.) That is painful stuff!
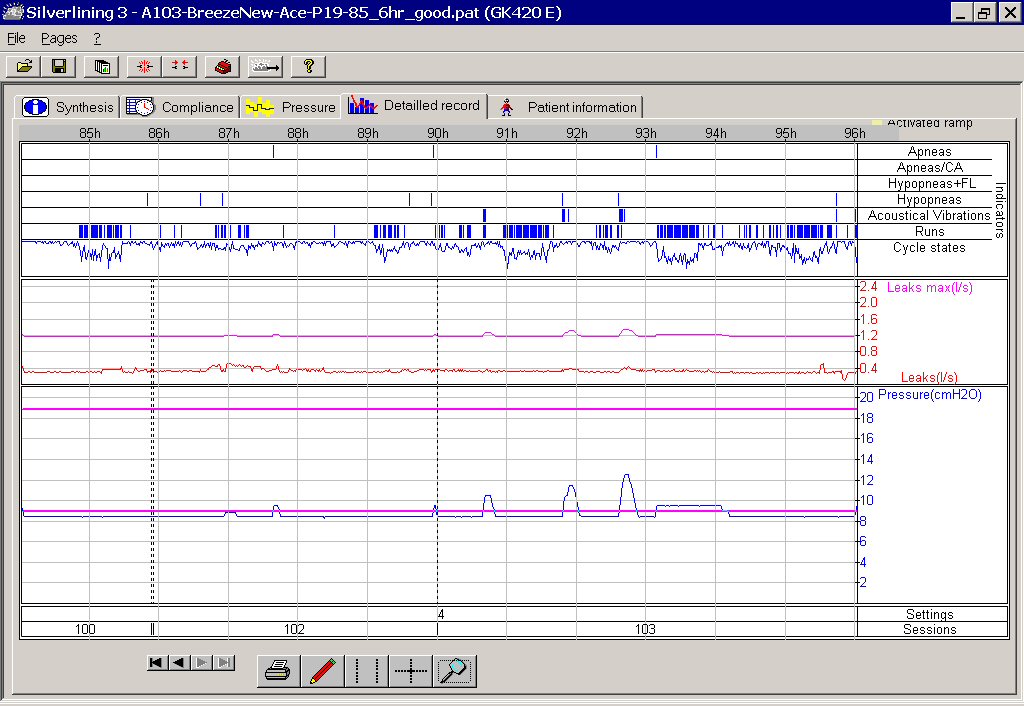
Compare that with the next screenshot, after SWS looked at my graphs and suggested I turn IFL1
OFF... leaving only IFL2 "on". In this picture, the pressure range was still set to allow a top of 19, but now the machine behaved beautifully, easily interpreting my shallow breathing and no longer futilely running the pressure up to the top. The pressure stayed down on 9 most of the two and a half nights shown in the graph. The pressure went up a bit from time to time to deal with things, just like it's supposed to, but it never had to go above 11 and 12 on two occasions. Nothing like the 17, 18, 19 it was wildly running up to when IFL1 was "on".
No problem with IFL1 turned "off", IFL2 left "on"
For most people using the 420E, the defaults of IFL1 "on" and IFL2 'on" can be left as they are - no problem. I hasten to say that, before 420E users think, "OMG, maybe I should turn off IFL1!!!" For me, IFL1 "on" didn't work well, but it would be fine for most.
IFL1 "off", IFL2 "on" - that was the right combo of advanced triggers for me. Perhaps my particular breathing pattern is a rare oddity for the 420E to have to try to deal with. My "shallow breathing" may not have even been the only factor that was confusing the machine. Other shallow breathers probably have no trouble at all with both IFL's left "on". Maybe there's something else about my particular breathing pattern that threw a cog in the wheel and confused the machine in my case
Interestingly, later I got a second machine (got a good deal, so privately bought a 2nd machine for a back-up.) I had quite a bit of trepidation about trying the second machine, as it was not a 420E, which was now behaving so perfectly. The second machine was a REMstar auto. I wondered if the REMstar would also misinterpret my breathing pattern and take off up into the stratosphere...in which case I'd be out of luck, because the REMstar has no separate controls for IFL1, IFL2, etc. So, I cautiously set the upper limit of the REMstar at 16, "just in case", for my first night trying it. Happily, the REMstar handled my breathing pattern fine and behaved itself, never going up anywhere close to 16.
I get equally good treatment with either machine. But, think about this for a moment. What if I had not had the software to see what was happening? Or knowledgeable posters on the message boards, to turn to for advice? I'd have figured, "Well, gee, it sure does take a high pressure for me." Or perhaps I'd have even thought, "Autopaps must not be the kind of machine I should have." Sound like what a doctor who is against autopaps in general might say? heheh
Do I think a doctor, even a "sleep" doctor, could have looked at my initial graphs and figured out what was going on with me and my 420E, much less known what to do about it? I seriously doubt it. Most doctors are not a bit interested in the nuts and bolts of these machines. I credit every bit of good treatment I've enjoyed to the experienced people posting on the message boards.
{kind=link}
{kind=link}