Page 2 of 3
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 3:13 pm
by Windsurfing_Steve
BlackSpinner wrote:
If you get any flack from the doctors, ask them about diabetics, if they suggest that diabetics not test their insulin levels. They test and adjust their insulin levels all the time. You can kill people with insulin, you can't kill people with air, you can however damage people if their settings are to low to treat their OSA.
Exactly BlackSpinner. I came to this forum because I was not getting answers from the Doctor when I called him, he said to just to give it time. When I mentioned the PVCs the doctor's comment was that we all have some. He did not have Steve's file and did not remember that because of the PVCs this very doctor ran over to Steve's cardiologist in alarm. I came here to see if you all could help. Steve and I are both excited about tonight and if he does better.
The doctors summary went like this:
"The oxygen saturation when awake was 96%. The cardiac rhythm was sinus. Frequent PVCs were seen during wakefulness and during sleep. There were periods of trigeminal PVCs. He had 112 beat run of ventricular tachycardia at a rate of 150 beats per minute. This occurred at epoch 203. At the time he was sleeping on his back in REM sleep and Demonstrating his obstructive sleep apnea."
The above is what has us motivated to get rid as many of these apnea's occurrences as we can and then go from there. Maybe one of those Oximetry devices would be helpful. That way we would know more about what is happening? Any advice on that? We do know that during the sleep study his oxygen level or SpO2 fell to 88%.
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 3:16 pm
by Windsurfing_Steve
Thank you. I got as far as getting the .jpg and tried everything to get it inserted. I will try photo bucket and can see how that would work.
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 3:29 pm
by Julie
Another consideration is whether or not he's sleeping with his mouth open and/or on his back... the latter will provoke more apneas than other sleeping positions, and the former means he's not getting treated if the cpap air is going out his mouth instead of down his airway... which means trying a full face mask like the Quattro FX or Hybrid could be worthwhile - so he can then breathe normally but not lose the air.
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 4:19 pm
by Pugsy
When you use Photobucket there is a box with url addresses in it....copy the last line in that box and paste it here on your forum message. It will show up as code..that last line includes the IMG brackets so normally nothing else is needed.
Use the preview button to see if your image shows up.
The AHI is predominately central. Until I see a report to see where the pressure wants to go...I don't think that increasing the minimum is the way to go...I think decreasing the maximum might be a better thought...but I need to see the reports first.
I don't know that your husband would be like this guy here( see my link) but he had higher centrals..almost no obstructives and also thought he needed to increase his pressures when reducing was the best way.
When I see centrals...and not many obstructives...until we know for sure that pressures don't make the centrals worse...I don't recommend increasing anything. Last I checked the links were still active. It is an Encore report but I think you will be able to see what we are talking about well enough.
viewtopic.php?t=68846
If someone is having centrals because of the pressure (and we can't explain them away as awake events or something) then using APAP with a wide range may not be the best way to go. Instead APAP with narrow range or cpap might be better.
I don't think increasing minimum to 7 would really hurt anything but I don't think you will get the results you desire because centrals can't be fixed with an increase in pressure (and could potentially cause more centrals) and his obstructive index is already acceptable.
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 5:02 pm
by Windsurfing_Steve
Pugsy wrote:
If someone is having centrals because of the pressure (and we can't explain them away as awake events or something) then using APAP with a wide range may not be the best way to go. Instead APAP with narrow range or cpap might be better.
I don't think increasing minimum to 7 would really hurt anything but I don't think you will get the results you desire because centrals can't be fixed with an increase in pressure (and could potentially cause more centrals) and his obstructive index is already acceptable.

Whew, that worked. Above is part of the report from last night. I am not sure exactly what you may need so will start here. When he had the sleep study without a CPAP he had 2 centrals and so with the machine the centrals are way up and the obstructives are down. Here are the numbers before CPAP and with only 5 hours sleep. 5 obstructives apneas, 2 central apneas, 44 hypopneas and 17 RERAs. Yielding an AHI of 9.5. He was not on his back much for the sleep study as I had him trained not to sleep on his back as he would stop breathing and it was scary.
I can easily include more from this report if you let me know which part would be helpful.
Donna
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 5:31 pm
by Pugsy
Windsurfing_Steve wrote:Here are the numbers before CPAP and with only 5 hours sleep. 5 obstructives apneas, 2 central apneas, 44 hypopneas and 17 RERAs. Yielding an AHI of 9.5
These are pre cpap machine numbers...mild OSA base on numbers.
What is/was the AHI and the breakdown from the report you showed the screen shot above?
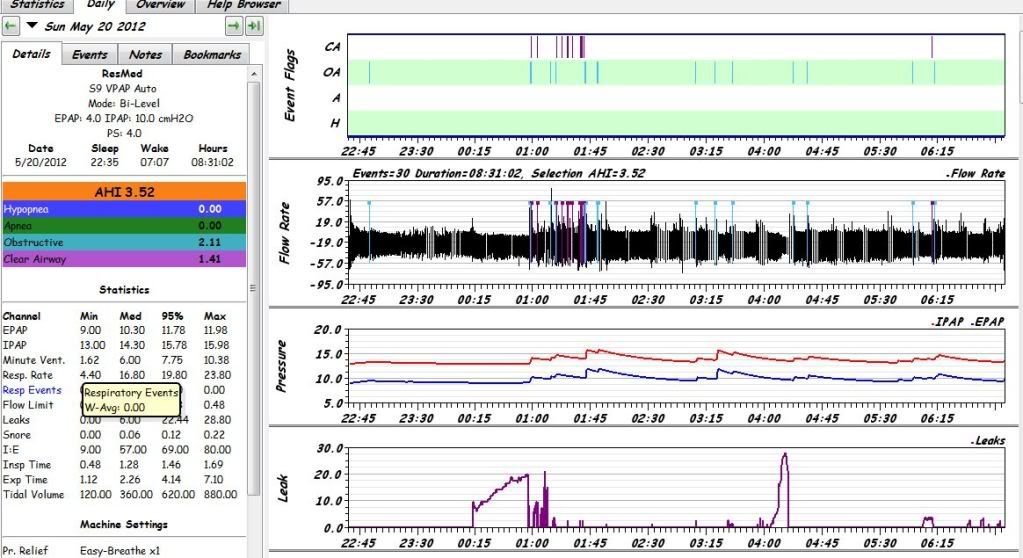
Can you get me a screen shot of the Events graph, flow graph, the pressure graph and the leak graph. You can get them all on one screen shot. It may be large but that is okay. Might need to resize the graphs just a little...hover mouse over the bottom line of the graph till you see a little short double line then drag upwards just a little to reduce the height of the graph.
You can go to Preferences tab in SleepyHead then graphs tab and turn off the AHI graph and mask pressure graph which will then let the Event graph, flow graph, pressure line graph and leak line graph show up on one image.
So I can see this sort of image in one screen shot. If you can't figure out how...that is okay...as long as I can see the 4 graphs I mentioned.
Here is an example of what I mean. It is a large image and part of it may seem to be cut off from viewing...just right click mouse over the image and choose "view image" and you should be able to see the entire report. It ends around 7 AM.
One of my reports..the cluster of events..I was awake at that time. Extreme nausea but didn't turn machine off or get out of bed.
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 5:50 pm
by Windsurfing_Steve

I think I did everything you asked. On a major learning curve here. Yes, we have understood that the OSA numbers indicate a mild problem. Again, he is experiencing heart arrhythmia from even a mild OSA. But then of course we may be getting to this earlier than some.
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 6:41 pm
by Pugsy
Got it. That helps a lot. Thank you.
The obstructive component to your husband's sleep apnea is fairly well treated. Huge improvement over pre cpap machine.
I think you can see that. Could you trim those obstructive apneas and hyponeas down a bit more...I don't know. Zero events is an unrealistic expectation though a few lucky people manage to get there. I understand your concern.
I will offer my thoughts on what I might do or what I might talk to my doctor about here if this were my report. I will try to explain why I think the way I do. My thoughts are just that...my thoughts. There is a lot we don't know and can't know from the data that we have available here. My very first suggestion....bring this report to your doctor's attention.
I see more centrals than I would want to see on this report. Now these machines don't know if we are asleep or not and they will flag events when if a person was in a sleep lab setting the sleep tech would look at the other data available (EEG for sleep brain waves, thoracic effort belt, and did something get flagged due to just turning over in bed) and determine if what is shown merits real concern or does it get tossed aside. We can't do that with what we see.
It is normal to have centrals during sleep onset and sleep stage transition. It is normal to have centrals when we just turn over in bed sometimes because often we hold our breath when we turn over in bed...we just don't realize it.
A central is a cessation of air flow and the airway is open. Hold your breath for 10 seconds and that meets the basic definition of a central....no air movement for 10 seconds but airway is open. The machine doesn't know that you held your breath on purpose. It just calls them like it sees them based on air flow information only.
So when we see centrals and there really wasn't any history of centrals during a sleep study...2 centrals is nothing...then we wonder if these are real or if they are turn over in bed hold your breath central or sleep onset central which would be normal and not warrant concern. So a few of these every now and then is no big deal and even if we don't know for sure or not...since there aren't very many of them then we don't worry.
Now there are a few people who actually happen to not have any significant centrals in their pre cpap sleep studies and once they get on the machine they start developing centrals. I think I read maybe 10 to 15 % of people might develop centrals when there weren't any centrals before. I am not saying that your husband is one of those people and I am not saying he isn't at this time. We simply don't know from this data.
I do see an increase in centrals (let's assume not awake centrals or sleep onset centrals for the moment) when the pressure nears 10 cm. The machine will NOT increase the pressure in response to any perceived centrals so we assume that the increases are because of some obstructive event precursors. So for some reason the machine wanted to go to 10 cm and a little bit of the time higher. Whatever the cause..it seemed to have done a good job as there are minimal obstructive events present.
If we didn't see the centrals....I would say a little increase in the minimum pressure might reduce a few more of those obstructive type of events. 4 minimum is really a low pressure and a small increase would hurt nothing.
I doubt that increasing the minimum a little will make any difference in the centrals IF they are even related to the cpap therapy itself but I don't know. No one knows for sure by just looking at a single report here.
Did your husband have multiple awakenings that might explain some of those centrals? I see one break in therapy line so I know at least once he woke up and turned off the machine. Were there other times where he woke up and just laid there and maybe tossed and turned a bit? See where I am going with this...if he reported some awakenings some of those "centrals" might not even be a real central in the sense that they warrant concern.
If they are related to pressure...then limiting the maximum pressure down to a level where centrals aren't triggered by pressure would be what we would normally look at trying to do...and still have to balance the need for some pressure to deal with the obstructive side of things. Sometimes it is a workable solution and sometimes a different machine is needed.
So I know I have thrown a lot of my thoughts out at you. I am a bit of a maverick with my own treatment but I tend to be conservative with my thoughts to others especially when they are directly under a physician's care and very new to therapy AND especially when I see more centrals in a report than I would like and I don't know yet if we can explain them away with sleep onset or turn over in bed centrals. If it were my report...I would limit the max at 10 and use minimum of 6...and see if the maximum limitation allowed any more obstructives and look to see if the centrals reduced. If no increase in obstructives and no decrease in centrals..then limit the max to 9...see what happens if I couldn't explain away the centrals.
Like that one example of my report I showed you. I know for sure I was awake and I totally disregard anything I see during that time frame.
If I had a doctor I was working with...he would be the first person I called when I saw these reports if I was sure I was asleep when those centrals showed up. He for sure needs to know about these centrals. We don't treat centrals with an increase in pressure because it might make things worse. We don't go changing things willy nilly when we see more centrals than are acceptable until we know for darn sure that they do not warrant concern.
Hope I haven't confused you too much. Would an increase in the minimum to 7 hurt anything? Probably not because the machine spends most of the night above that anyway right now. Would that increase maybe limit the hyponeas? Maybe it might prevent a bit more of them. Might not. It is doubtful that you can prevent them all but a reduction from an AHI of 9 down to around 1 (just the obstructive components) is a good sized reduction. We sort of have to set the central component off to the side while evaluating that part. Over a 6 hour period...9 per hour times 6 hours is 54 events and reduced to 1 per hour is 6 events...it is a substantial reduction.
You need to talk to your husband's doctors about your concerns both about the residual obstructive component that concerns you and the centrals...which are of a concern until they are proven to be of no concern.
Re: New with two weeks on CPAC
Posted: Sun Jun 17, 2012 7:31 pm
by Windsurfing_Steve
Thank you Pugsy. I read this and then Steve read this. We are on a big learning curve but your words are very understandable. We now are taking the Centrals much more seriously and thank you for taking the time to write this down for us. I will read again in the morning and see what the readings are. Thank you again.
Donna and Steve
Re: New with two weeks on CPAC
Posted: Mon Jun 18, 2012 5:29 pm
by Windsurfing_Steve
I just read on another thread that we can look in the event tab and see how long events are lasting. I just looked and see numbers and am wondering what these numbers mean? These are CA numbers and do they seem like normal numbers to see, I mean if you have CA events?

Re: New with two weeks on CPAC
Posted: Mon Jun 18, 2012 5:55 pm
by Pugsy
CA means Clear Airway...open airway cessation of breathing..in other words...central.
When SleepyHead was first developed it was for Respironics machines which uses the terminology...clear airway event..instead of central. They preferred to call them clear airway...ResMed is comfortable calling them centrals.
The number in parenthesis after the time of the event is the duration of the event in seconds.
Resmed machine compatibility was added to SleepyHead much later but the terminology was left at clear airway because technically that is what a central is.
Re: New with two weeks on CPAC
Posted: Mon Jun 18, 2012 6:06 pm
by Windsurfing_Steve
Pugsy wrote:CA means Clear Airway...open airway cessation of breathing..in other words...central.
When SleepyHead was first developed it was for Respironics machines which uses the terminology...clear airway event..instead of central. They preferred to call them clear airway...ResMed is comfortable calling them centrals.
The number in parenthesis after the time of the event is the duration of the event in seconds.
Resmed machine compatibility was added to SleepyHead much later but the terminology was left at clear airway because technically that is what a central is.
Thank you Pugsy. Yes, I understood the Clear Airway part. I am wondering about the numbers and you have said that they are seconds. So now I wonder if Steve's numbers where he has a clear airway event lasting 23 seconds. Is that a long event or is that a typical number to see?
Re: New with two weeks on CPAC
Posted: Mon Jun 18, 2012 6:17 pm
by Pugsy
Any event has to last at least 10 seconds to be flagged...9 seconds and it doesn't get flagged.
From what I have seen from other people and myself..23 seconds is not unusual at all. Hold your breath for 23 seconds. It is easily done. Once in a while it likely won't cause distress and is really easy to do unless someone has lung issues. Hold it for 23 seconds...once a minute for 5 minutes straight...you will likely feel the effects.
I had a 53 second event not long ago...that was rare ugly one. Up to 30 second events are very common for me. I do see longer ones but they are rare.
Some people have reported events lasting longer than a minute. Somewhere between 10 and 40 second duration are likely very commonly seen.
Duration is of course a concern but frequency is also a concern..even if the frequent events are of shorter duration. If they are back to back and nearly on top of each other then the cumulative effect is just as detrimental as a nice big long event all by itself.
Re: New with two weeks on CPAC
Posted: Mon Jun 18, 2012 6:23 pm
by SleepyToo2
Based on my numbers, it is fairly long, but I have had events of 35 s in recent nights. Many are much shorter. The key for me would be to see if you can find out whether there is a relationship between the breathing events and the arrhythmias. That would be another thing worth reporting to his doc. Good luck in your search for answers.
Re: New with two weeks on CPAC
Posted: Mon Jun 18, 2012 6:44 pm
by Windsurfing_Steve
Pugsy wrote:Any event has to last at least 10 seconds to be flagged...9 seconds and it doesn't get flagged.
From what I have seen from other people and myself..23 seconds is not unusual at all. Hold your breath for 23 seconds. It is easily done. Once in a while it likely won't cause distress and is really easy to do unless someone has lung issues. Hold it for 23 seconds...once a minute for 5 minutes straight...you will likely feel the effects.
I had a 53 second event not long ago...that was rare ugly one. Up to 30 second events are very common for me. I do see longer ones but they are rare.
Some people have reported events lasting longer than a minute. Somewhere between 10 and 40 second duration are likely very commonly seen.
Duration is of course a concern but frequency is also a concern..even if the frequent events are of shorter duration. If they are back to back and nearly on top of each other then the cumulative effect is just as detrimental as a nice big long event all by itself.
Very interesting. I will be watching these number. This Sleepyhead is a way cool little program. Did you create it Pugsy?