Re: ASV users: the everything ASV thread.
Posted: Tue Jan 22, 2013 9:19 pm
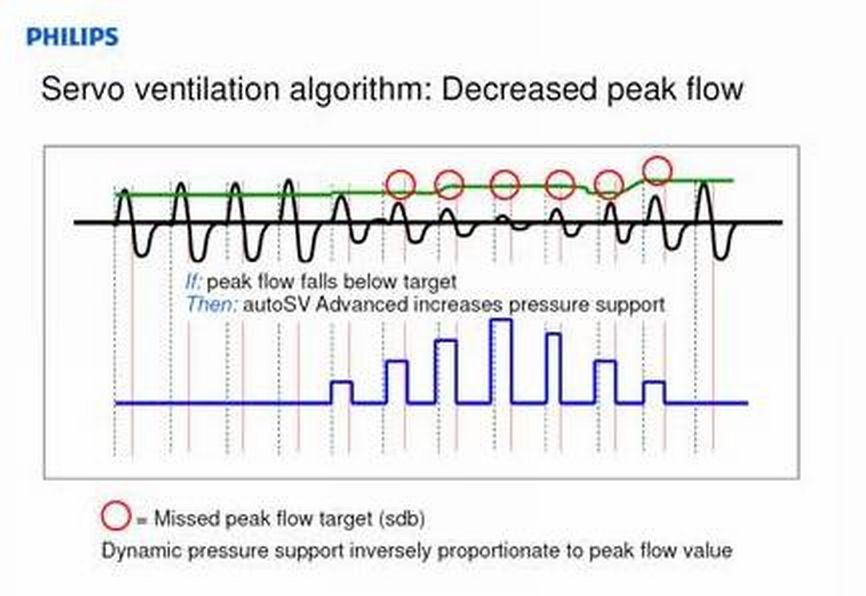
I agree. The ASV part of the algorithm above is probably not going to treat UARS---based on RERA occurring before sufficient volume reduction has occurred. And I don't see where the EPAP-adjusting treatment arms in either brand ASV will avoid UARS RERA's significantly better than ordinary APAP algorithms. As a result, I envision Dr. Krakow's UARS patients still leaving NPSG with high PS min values. I think Dr. Guilleminault still prefers ordinary CPAP for his UARS patients. I suppose two germane questions for any UARS patient is: 1) where is threshold of arousal relative to perfect sinusoid, but more importantly 2) what pressure settings are sufficient to avoid RERA? Unfortunately, iatrogenic problems can offset the intended benefits of those high pressures.mollete wrote:So it strikes me that it would only work when one's baseline peak flow is normal (and one has real "peaks"):-SWS wrote:Respironics ASV targets 95% of recent-averaged peak flow...
However, if one's baseline is flow-limited, the most one could hope for is 95% of that, which may not attain "normalcy".
Perhaps one could hope that the ASV would see a failure to respond to PS and identify the event as obstructive-- however, the PR ASV response to obstruction is raise EPAP (that's the only thing it can do to correct the underlying issue), and not simply chase it all night long.
Which is why I contend that an AutoAnythingElse algorithm is better suited to attack obstructions (i.e., look for snores and flow-limitations, positive response to pressure increases, etc.).