In attempting to understand the concept of Flow Limitation (FL), and the new ResMed measure, Fuzzy Flow Limitation (FFL), I believe it is important to review some of the components in the document presented by LoQ (op. cit.). In that document, it appears that FFL is actually composed of at least 3 measures:
Wave Form Shape (with accent on "M" and "Chair" shapes);
Dynamic Tidal Volume, expressed as Ventilation Ratio (VR); and
Inspiratory Time, expressed as a fraction of the duty (entire respiratory) cycle, or T
i-on-T
tot Ratio (TTR).
It is critical to note, however, combinations of these components may either enhance or ameliorate FFL, as noted in the four tables. For instance, no matter how vicious an "M"-shaped waveform is, if VR is high or very high, the algorithm says it's NBD.
Additionally, snoring, leaks, an extraordinarily long inspiration or expiration, and level of pressure are also accounted for, which, "IMHO" make this algorithm
very clever, not only preventing pressure attacks on suspect waveforms, but identifying (indirectly) arousals and attacking RERAs with reasonable accuracy (more later).
So if the FFL isn't simply a measure of "flatness", in order to properly analyze this, we need to look at the aforementioned "number" associated with FFL (you can see this by "mousing over" the waveform, or use the methodology discussed elsewhere to edit ResScan and add Values to the graphs):
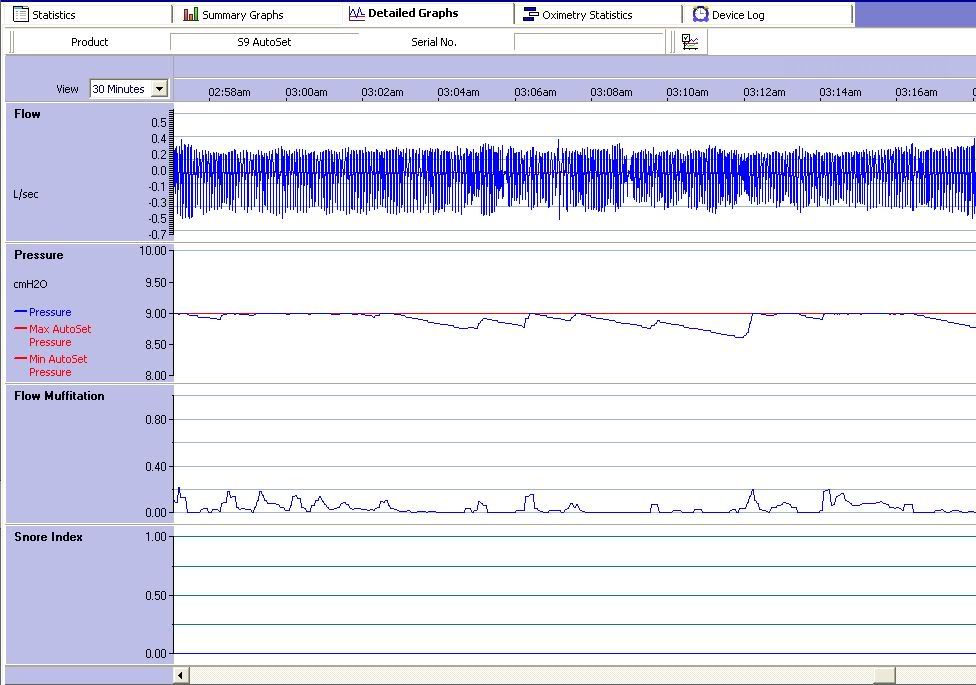
In this version of MuffScan I've also added numerical value to snoring, another discussion point for later.
As noted by gvz, it is
extremely important that one make a back-up copy of any config files before you edit them. Make note of the file name, and also be sure it's called something that you'll be able to find later. Otherwise, you will end up in the same boat as Muffy, who labels her files such things as "I'llRememberThis" or "Thursday" or "Important", and stubbornly refuses to believe that she will not, in fact, remember what day it actually is much less what a file called Monday (or Monday(1256). She does that a lot) goes to.
BTW: I think I'll hold off on "fuschia", at least for the first part of this discussion. That might be a little much.
Besides, the Fuschia File was called...
...was called...
...is today Wednesday?