I'd like to add some real life data to this interesting thread. My own nightly desats come in groups every 2 hours, probably in REM sleep, for a typical duration of 30 minutes. A typical Oximeter report for the first two hours of my night
without CPAP looked like this

This cycle repeats more or less over the night.
Having done with mouth leaking and mask issues (using the Hybrid with no leaks) I can finally try how different auto CPAPs deal with this pattern.
The CPAP I'm currently using is the DeVilbiss IntelliPAP. My pressure range is set to 10-18 cmH2O.
NotMuffy, I know that 10 cmH2O may be too low to start with but I can't set the minimum any higher due to aerophagia (I tried).
(BTW for other discussion - the IntelliPAP reports expiratory puffs with a taped well-sealed mouth. I have no idea how it's possible)
I expect that once events start, the auto CPAP would quickly up the pressure to deal with the events, then slowly lower it when done, until the next round.
Sadly, the DeVilbiss IntelliPAP can't do that.
With its default settings, once problems start, the IntelliPAP would ramp up the pressure 2-3 cms over the course of 30 minutes.
This is a joke and does not deal with my breathing problems at all.
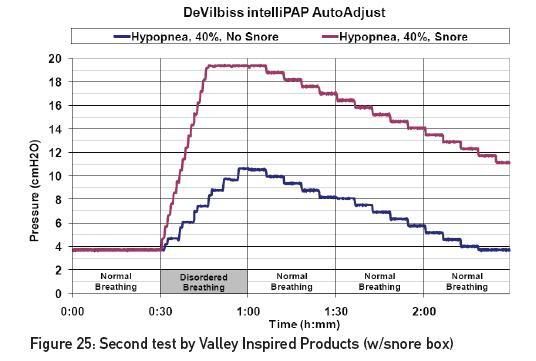
To increase sensitivity, as suggested here by DeVilbiss Marketing, I adjust the apnea % to 0% so that all events would be recognized as hypopneas. The IntelliPAP response to apnea and hypopnea is identical so apnea definition only changes the report but not the response. I also adjust the hypopnea % to 30% reduction for 6 seconds. These settings make the IntelliPAP as sensitive as possible.
What happens? indeed, the IntelliPAP raises the pressure up to 18 cms, much higher than the default settings.
However, it still takes the same time to get there, about 30 minutes, which is a useless solution to a 30-minutes hypopneas attack.
Nightly pressure with aggressive settings:

Although DeVilbiss claim that the AutoAdjust can raise pressure 1 cm every minute rate of change (a rate not very fast by itself), even with the most aggressive settings I have not seen it raise the pressure more than 1 cm every 3 or 4 minutes. That's awfully slow. By the time the pressure was raised from 10 to 18 the events are done.
Also, with aggressive settings the IntelliPAP identifies hypopneas while awake and raises pressure accordingly. I used 20 minutes ramp at the minimum pressure to avoid this problem. This is the first time I found use for the ramp function.
DeVilbiss could
easily fix the AutoAdjust algorithm with a
software upgrade, for example using an "aggressiveness" parameter or by recognizing flow limitations as everyone else do. I hope they do, because hardware-wise the IntelliPAP is very nicely built.
However, until they fix it, the AutoAdjust algorithm do not provide good therapy for people like me, Jayjonbeach and likely many other people who have periodic hypopneas that suddenly appear and disappear, say in REM sleep.
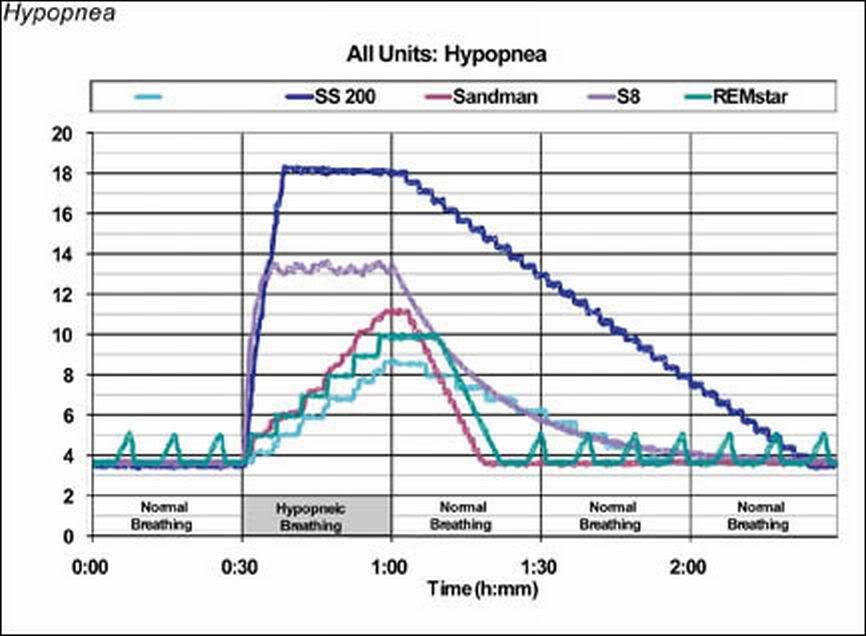
I plan to try out other auto CPAP and will update here.