Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Posted: Fri Jun 11, 2010 7:33 pm
Hi unadog, Are you suggesting that the Adapt SV might be sensing ballistodillionographical artifacts?unadog wrote:2) dillion...
A Forum For All Things CPAP
https://www.cpaptalk.com/
Hi unadog, Are you suggesting that the Adapt SV might be sensing ballistodillionographical artifacts?unadog wrote:2) dillion...
Hmmm...maybe you have found the key to my ASV PSG stutters: sleep dilloniated breathing (SDB)?SleepingUgly wrote:I think he meant what he said...
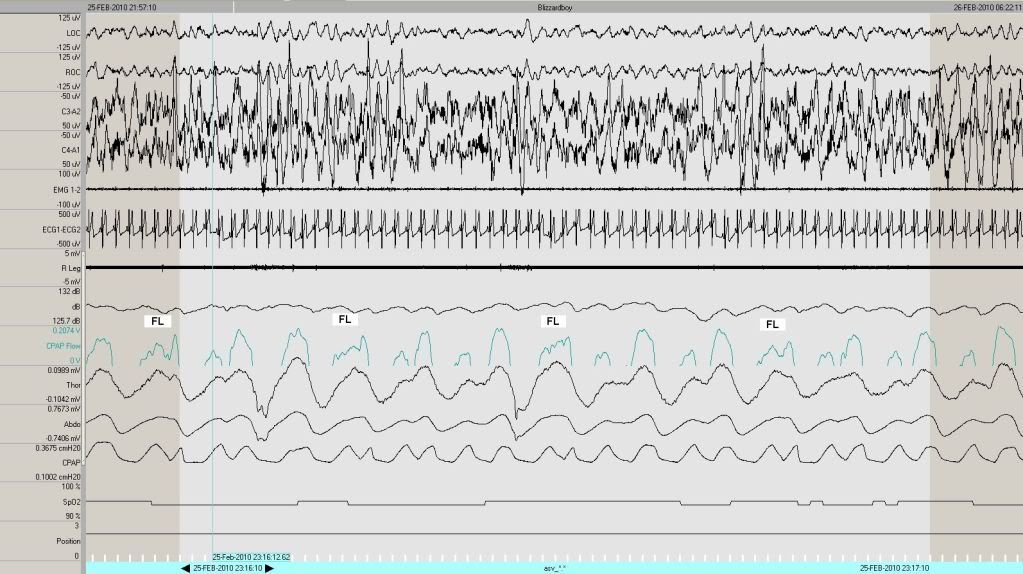
At the risk of microanalyzing your microanalysis, and keeping in mind that this is offered as a possible explanation for something you did once (recurring theme of solitary events that don't need to be bludgeoned to death), if the CPAP Flow is clipped at 0.0 volts to allow only the + portion, then this should expose only the inspiratory limb of the breath:blizzardboy wrote:I am trying to understand what the algorithm is attempting to acheive during these periods of "double hitting". I suppose, given the flow-metering nature of CPAP, that mid-inhalation the machine senses a partial exhalation followed by the completion of the inhalation cycle i.e. stutter, thus demonstrating the rapid nature of the ASV response to respiratory variations and its charter to maintain tidal volume.Muffy wrote:Just about every breath gets a double hit.
Exactly!blizzardboy wrote:Are you suggesting that the Adapt SV might be sensing ballisto...graphical artifacts?
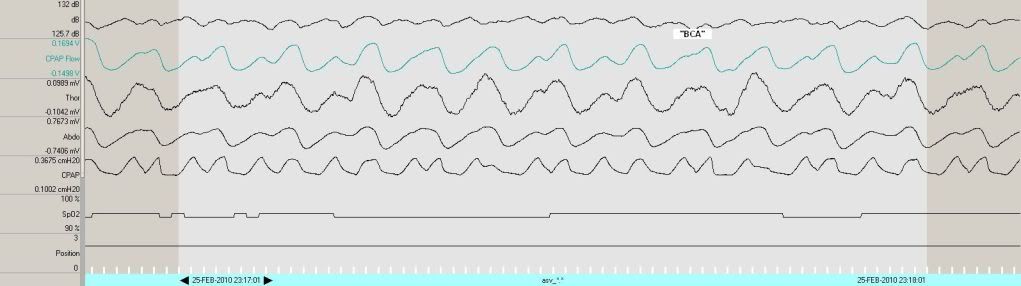
Hi Muffy, ('scuse me if I'm being obtuse) the dB channel was recorded with a microphone located above my bed and I am sure I remember the Adapt SV having that unit attached to the back and wires disappearing into the wall. Very nice to see the inhalation portion of the flow channel - thank you, clearly shows the likely source of the supercharged resp rate, eh?Muffy wrote:Keep in mind that I don't believe this to be a ResControl signal because of the reasons previously mentioned (and because of the behavior of the Snore Channel, I believe they employed a PTAF2 system), and if so, doesn't represent in the strictest sense what the AdaptSV actually "sees".
i.e. for the Adapt SV the interpretation of respiration status becomes tricky as the flow rate drops below some threshold (and further complicated by the presence of ballisto...graphics)?Muffy wrote:So anyway, what I think is happening is that you're having Flow Limitations that slow to the point where the AdaptSV thinks your flow has (briefly) ceased, switched to EEP, then back to IPAPwhatever nearly instantaneously. This completes a single inspiratory effort, but registers as a "stutter" vis-à-vis Respiratory Rate.
Hmmm...so is there a line up of usual suspects as perpetrators of these intrusions? Cheers,Muffy wrote:As a further aside, man, you gotta put some salve or something on that alpha intrusion.
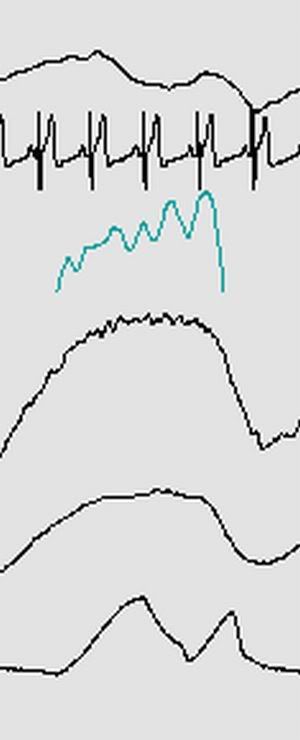
So we are seeing cardio ballistics coming through here, right?Muffy wrote:Exactly!
I doubt dB was taken from the microphone because filtering out the "snore" portion of the waveform results in a breathing waveform. This is most clearly seen in the obstructive apnea:blizzardboy wrote:Hi Muffy, ('scuse me if I'm being obtuse) the dB channel was recorded with a microphone located above my bed and I am sure I remember the Adapt SV having that unit attached to the back and wires disappearing into the wall.Muffy wrote:Keep in mind that I don't believe this to be a ResControl signal because of the reasons previously mentioned (and because of the behavior of the Snore Channel, I believe they employed a PTAF2 system), and if so, doesn't represent in the strictest sense what the AdaptSV actually "sees".
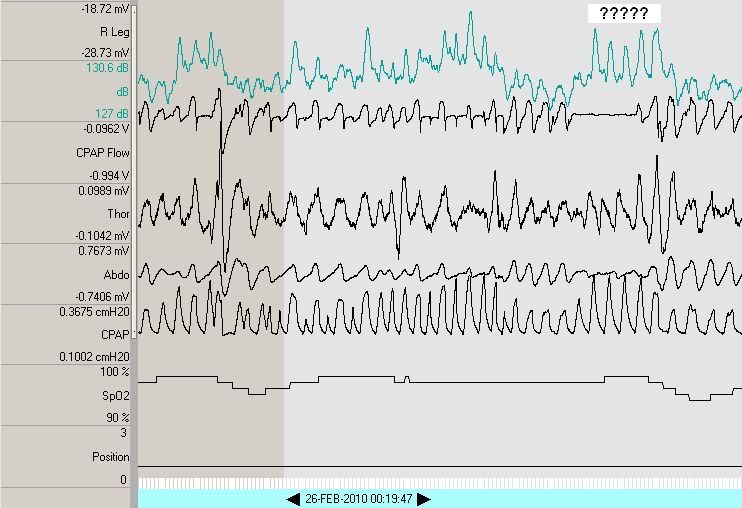
I've been thinking that the microphone was picking up the Adapt SV getting noisier as it ramped up the IPAP, hence the correlation between the dB and CPAP channels during these occasions. Did you manage to find your DOS 5 1/4"s to reinstall your OS?Muffy wrote:Rather, dB mirrors CPAP.
8-inch, actually.blizzardboy wrote:Did you manage to find your DOS 5 1/4"s to reinstall your OS?
Upon further reflection, that must have been what happened:blizzardboy wrote:I've been thinking that the microphone was picking up the Adapt SV getting noisier as it ramped up the IPAP, hence the correlation between the dB and CPAP channels during these occasions.Muffy wrote:Rather, dB mirrors CPAP.

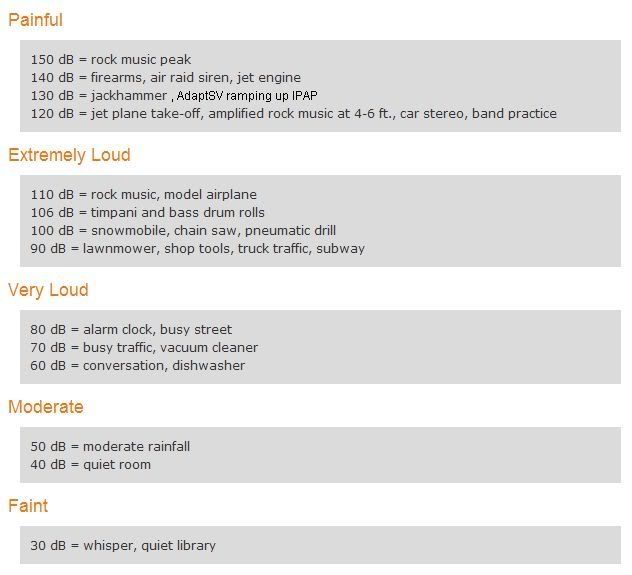
Ah, yup, good point...like I said:Muffy wrote:Upon further reflection, that must have been what happened...130db=AdaptSV ramping up IPAP
blizzardboy wrote:...('scuse me if I'm being obtuse)
It's an absolutely certain maybe.blizzardboy wrote:Very nice to see the inhalation portion of the flow channel - thank you, clearly shows the likely source of the supercharged resp rate, eh?
If you're talking about the respiratory rate thing, keep in mind that you did that once, and it had no clinical significance.blizzardboy wrote:i.e. for the Adapt SV the interpretation of respiration status becomes tricky as the flow rate drops below some threshold (and further complicated by the presence of ballisto...graphics)?
As you've probably noted through your research, the jury's still out on the clinical significance of alpha intrusion.blizzardboy wrote:Hmmm...so is there a line up of usual suspects as perpetrators of these intrusions?
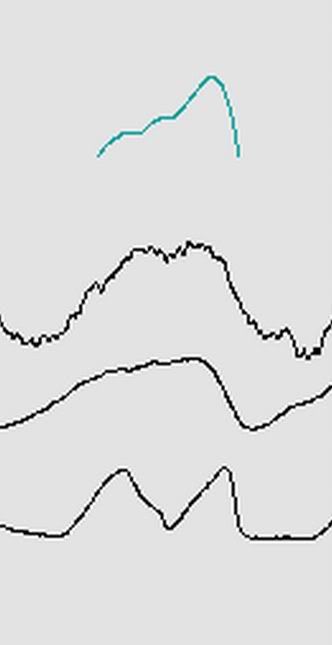
With a little bit of LP filter applied to that same BCA, andMuffy wrote:If you're thinking that ballistocardiographical artifact can mess up the algorithm, I doubt it. That waveform is undoubtedly filtered in machine analyses (in the same manner I have turned the snore channel into a breathing channel) so BCA is attenuated. We are able to see it now because I don't think that's a ResControl data channel.