Re: CompSA, Hypoventilation, PLMs, Bradycardia and Hypotension?
Posted: Wed Apr 14, 2010 7:41 am
The server dudes here at work block that site from me entirely.-SWS wrote:. . . to download the files. . . .
A Forum For All Things CPAP
https://www.cpaptalk.com/
The server dudes here at work block that site from me entirely.-SWS wrote:. . . to download the files. . . .
jnk wrote:The server dudes here at work block that site from me entirely.-SWS wrote:. . . to download the files. . . .
-SWS wrote:I just downloaded the file successfully. Not sure what went wrong the first time. I saw this erroneous average heart rate followed by the :I certainly wouldn't put hypoventilation, hypercapnia, bradycardia, or vagal events on the front burner or back burner based on that data. However, if I episodically returned wild swings in my home-measured BP, SpO2, or ASV data, then I'd take a close look at some of those possibilities. My understanding is that some cardiac and central symptoms can be highly transient---especially during onset of certain diseases.Average heart rate during sleep: 20
Number of Bradycardic periods: 0
I can't see your data. Did you have PLMs on the home study that you didn't discontinue Fluoxetine for? On the "real" study in the lab, the one that you discontinued Fluoxetine 2 weeks prior, did the PLMs cause arousals?blizzardboy wrote:Given that I apparently have a lot of PLMs I certainly would be interested to know what are the options for treatment.
Please try this link to see my PSG reports:SleepingUgly wrote:I can't see your data. Did you have PLMs on the home study that you didn't discontinue Fluoxetine for?
Sure, can't hurt, but I reserve the right to debate whether or not this is truly CompSAS at some point. The 11.02.2010 study was on ambient pressure (CompSAS is usually defined as the appearance of centrals with the addition of pressure) and their location could make them caused simply by sleep fragmentation (they are post-arousal) or due to sleep transition (dozing at the end of the night's sleep).blizzardboy wrote:Probably good just to give my body a good run on the ASV first. What do you reckon?




Yup, yup, yup...ASAP! I had lousy sleep architecture: skipping between S1 & S2, 2 mins of S3, no S4, no REM, AHI 62 all hypops, Sa02 went down to 83%, average heart rate 98 (yikes, I forgot this), no limb movement, normal EKG & EEG, arousal index=30 mostly resiratory; split-study sleep efficiency 99% (no numbers given in summary) & SaO2 +92%. I barely made it into the category of slept long enough for insurance to pay for my PSG. First 17-18 months with dataless CPAP, I slept thru the night; thereafter, wakeups every 90-120 mins. Still have wakeups; now that I have detailed data, tracking to see if these follow events, so far, some yes, some no. Hypersensitive to noise, light, movement (even air), temp changes, state of my chronic congestion (vasomotor rhinitis, allergies, chronic sinusitis), phase of the moon too maybe -- it's so very frustrating not to be able to stay asleep & being tired as a result. The more wakeups, the lousier I feel the next day. Since last Nov, my average AHI=1.4 with AI=0.1, some--maybe many--envy these numbers I know but these wakeups are wrecking havoc with my energy, alertness, sleepiness, cognition, mood regardless of how good they are. We all have our crosses to bear with SDB and right now mine seem to cluster around my variable congestion and these dratted wakeups. Oh, I also still have a ton of wt to lose; lost 57#, then stalled for a yr, gained back 12 over the last few months and can't seem to find the energy, time, or incentive to exercise regularly -- the excess wt isn't helping either. At least my bloodwork's better, no more compensation as if I were living at high altitute so I assume I'm not desating much.Muffy wrote:...We need the Muffy Guide to sleep hygiene....
Unless it falls on his head, of course.Muffy wrote:Sure, can't hurt . . .blizzardboy wrote:Probably good just to give my body a good run on the ASV first. What do you reckon?
Or did that get addressed, and I just got lost again? Sorry if I did.blizzardboy wrote:. . . using a CMS-60C ABPM I find that my blood pressure drops to 80/43 during the night . . .
I concur wholeheartedly. I was very hesitant to go on fluoxetine. I would probably been even more concerned about taking the types of drugs that I have seen listed for treating PLMD. I think I would like to ensure that I have exhausted as many health, diet, exercise, relaxation, etc options before I start going down the meds path. For, as you testify to, tampering with one's biochemistry can be a bit of a Pandora's box.kteague wrote:Besides arousals, the body needs to rest during sleep. Your legs don't rest. I have found the chronic muscle and joint pain to be as limiting as the poor sleep, just in different ways. Do you have pain with yours? I just broke down and called my doctor today. As much as I dread another transition, the Requip is now causing more limb movement issues than it is fixing. Woke up last nite in the middle of a movement - lying on my side my arm was stretched straight up in the air like the hand on a clock pointing toward midnight. Enough is enough. These exaggerated movements aren't the PLMD, they're the side effect of the high dose of the med. This is not a path you want to take if it is in your power to avoid it.
OK. So how to improve architecture? I have cut right back on alcohol consumption. My diet is pretty good although maybe a little too high in carbs. My exercise levels are not satisfactory at present (exacerbated by fatigue related to sleep problems). I don't smoke. Maybe three coffees per day. No other recreational drugs. I have a new bed and mattress that seems to be comfortable for my body. I don't each much after 7:30pm, tend to be in bed no later than 10:30pm and usually sleep until 7:30am.Muffy wrote:...swarming with arousals. That's a lot of bad "sleep".
Muffy
I scored 55 on that high-tech sleep hygiene survey. 'Twould seem I am a moderately grubby sleeper.Muffy wrote:Here's a couple threads where sleep hygiene is discussed:
viewtopic/p472062/viewtopic.php?f=1&t=4 ... ne#p401345
viewtopic/p472062/viewtopic.php?f=1&t=4 ... ne#p372562
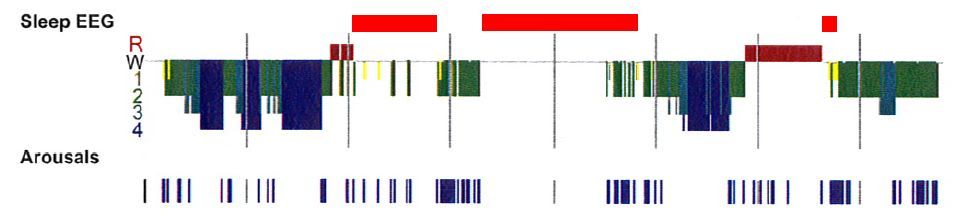
No sleep architecture page was shown/given to me following my first PSG.Muffy wrote:Is there another page of the home study showing the architecture?
I can see that my sleep architecture is not necessarily helped by the ASV, but isn't it still worth having an ASV assist in ventilating me during centrals until the cause of arousals is identified?Muffy wrote:It makes no sense to hammer a post-arousal central with an ASV because the damage is done.
I have been receiving CBT regularly for a couple of years now. Profoundly helpful to me.Muffy wrote:If everything gets optimized and sleep architecture remains poor, I would consider the use of Cognitive Behavior Therapy.
Ditch fluoxetine, eh? I'll talk to my GP about options less likely to increase PLMs. Elsewise: Get properly fit again? Work outdoors? Plenty of sunlight?Muffy wrote:Consider changing/getting rid of the ADM.
Muffy
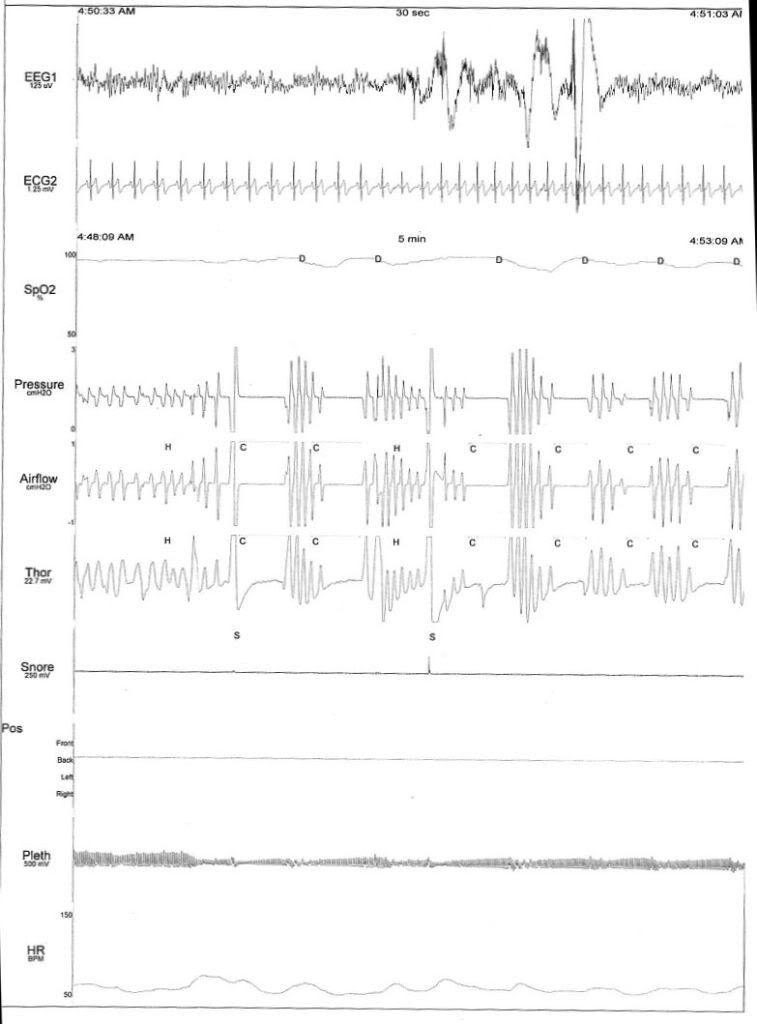
Maybe not? Did you notice that the EEG/ECG traces are on a different time scale to the others? Does this change your reading?Muffy wrote:BTW, in the Epoch you presented from the HST:
(look back for picture)
you're awake. Throw out all those centrals.
Muffy