Page 16 of 26
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 9:07 am
by -SWS
Muffy wrote:I disagree with your disagreement. The CompSAS cycle is perpetuated by overshoot, so the key is not how it blows through the CA, but how pressure support drops back during the hyperventilatory period immediately after. That is the critical area. If this were not the case, then simple BiPAP with a backup rate would be successful in treating CompSAS and there would be no need for ASV.
Further, singular (or more specifically, isolated) central apneas are nearly always benign, and should be left alone.
Muffy
You know how I feel about these
disagreements. Respironics may have to rework their wording since they clearly state their BiPAP autoSV will automatically trigger a breath for a central apneic event (singular). Respironics never mentions anything about that machine's backup rate being reserved for multiples, cycles, or sequences of central apneas. They address periodicity patterns with fluctuating PS. But they never explicitly or implicitly claim to refrain from backing up singular central apneas with their backup rate.
They even use a
singular central-apnea case in their description of administering backup rate:
the BiPAP autoSV algorithm also calculates the patient's spontaneous breathing rate and will automatically trigger a breath should the patient have a central apneic event.
http://bipapautosv.respironics.com/how.aspx
So if the BiPAP autoSV refrains from administering its backup rate to singular central apnea events, I can't find that anywhere in literature. But I can find statements like the above describing
"a central apneic event" (singular) receiving that algorithm's backup rate.
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 9:14 am
by -SWS
Sorry about the side discussion, CROWPAT... I had better place your sleep hygiene answers on this page to make them easier for Muffy to work with:
CROWPAT wrote:1. You are truly a "long sleeper" and that's just how it's going to be (and if you were only sleeping 5.5 hours back when you were working, then that must have been hell)(Hey! Hell On Wheels! Wasn't that the nickname of an armored division?) 1st or 2d AD, I forget.
2. You are "oversleeping" and it's too much. Statistically, long sleepers tend to have the same morbidity/mortality as short-sleepers;
3. You have a sleep maintenance issue, and that 9 hours of DL time is really like 7 hours of sleep;
4. You have another medical issue(s) (like uncontrolled depression).
Can you get a clear copy of the graphs from 2006? I will try to get one.
Time for a sleep log:
http://www.sleepeducation.com/pdf/sleepdiary.pdf I downloaded it.
Do you take naps? Never.
See the receptionist for another appointment in 2 weeks.
Muffy
Got up, went out in 24 degrees, and walked for 30 minutes. Fog returned shortly after I got home, but no worse than usual.
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 10:53 am
by Muffy
-SWS wrote:So if the BiPAP autoSV refrains from administering its backup rate to singular central apnea events, I can't find that anywhere in literature. But I can find statements like the above describing "a central apneic event" (singular) receiving that algorithm's backup rate.
I didn't say it didn't, I said it shouldn't. My point is that not every central apnea needs to be bludgeoned to death.
Muffy
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 11:44 am
by -SWS
Got it... and I agree that a rare or isolated (brief) central apnea is perfectly benign. I'm not sure... But here's where our paradigms might turn out to disagree a bit regarding key objectives for this ASV machine's fluctuating IPAP peak:
The CompSAS cycle is perpetuated by overshoot, so the key is not how it blows through the CA, but how pressure support drops back during the hyperventilatory period immediately after. That is the critical area. If this were not the case, then simple BiPAP with a backup rate would be successful in treating CompSAS and there would be no need for ASV.
Once in that cycle, the recurrent moments of biological undershoot are genuinely problematic as well.
This Respironics algorithm fluctuates IPAP peak between the bounds of IPAP min and IPAP max for both halves of an oscilation-based respiratory controller problem: progressive biological overshoot cyclically interspersed with progressive biological undershoot. Accordingly, the algorithm drops toward IPAP min during those moments of biological respiratory overshoot. I agree that is in part key. However, strategically it is only half-key. And IPAP peak cannot actively or instantaneously minimize or
subtract that biologically-produced volume over-flow simply by dropping IPAP peak. Rather, IPAP peak simply avoids exacerbating that biological over-ventilation by stepping out of the way or minimizing mechanical ventilation.
By contrast, the
other fluctuating IPAP "half-key" (when IPAP peak proportionally moves toward the IPAP max limit)
actively or additively assists ventilation during those moments of biological undershoot. Additional timely and proportional flow is generated by the machine to assist with biologically generated flow being under-target. So I view the IPAP peak upswings as assisting with proportional machine-generated flow, but the IPAP peak downswings as essentially stepping down to avoid mechanically exacerbating those moments of biological overshoot.
ASV's Proportional Assist Ventilation is an inherently bipolar proposition: active ventilatory assistance for increasingly deficient biological flow during IPAP peak's progressive upswings; but avoidance of biological exacerbation as IPAP peak proportionately stands down with its pressure support during progressively developing cycles of biological overshoot.
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 7:40 pm
by dsm
Muffy wrote:
<snip
ASV technology is designed to fix a cyclical central pattern. It does not "fix" any singular central apnea per se.
<snip>
Muffy
Muffy
Excellent info on clarifying central types & their relevance - very easy to forget that aspect. But re the above point, wouldn`t the timed mode feature of an ASV address any isolated central s ? was also thinking that the flow targeting algorithm would try to smooth out a sudden dip below current flow. Both being to switch to ipap & boost ipap (reason I ask is I measured av 3 CMs boosts on my machine repeated for 3 breaths if simulating a central).
DSM
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 8:28 pm
by -SWS
I believe Muffy's clarified point above was that the ASV machine's design intent was never to fix a few isolated benign central apneas. The original comment really had to do more with matching the right patient to the right machine. Muffy succinctly clarified later on that the comment was not to say that the ASV machine is algorithmically incapable of responding to individual central apneas.
The machine's target application:
Respironics FAQ wrote:What is the BiPAP autoSV device used for?
The intended use is: To provide non-invasive ventilatory support to treat adult patients with OSA and Respiratory Insufficiency caused by central and/or mixed apneas and periodic breathing.
http://bipapautosv.respironics.com/faq.aspx
Periodicity or cyclic central apneas are not a target requirement above---since there are cases when non-cyclic central apneas
need to be addressed. The machine's backup rate will thus, by design, commence timely ventilation for central apneas either with or without cyclic characteristics.
But I agree with Muffy: a few isolated and benign central apneas are not at all what the ASV was designed to "fix".
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 9:04 pm
by timbalionguy
So this begs a slightly off-topic but pertinent-to-the-discussion question: If one finds that they will have to use a servo ventilator, how does one go about making the right decision the first time? Or is this something that your clinician pretty much has to decide? These are really expensive machines, and very few can afford one of each.
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Fri Dec 11, 2009 10:22 pm
by Guest
timbalionguy wrote:So this begs a slightly off-topic but pertinent-to-the-discussion question: If one finds that they will have to use a servo ventilator, how does one go about making the right decision the first time? Or is this something that your clinician pretty much has to decide? These are really expensive machines, and very few can afford one of each.
The right decision the first time would default to the VPAP Adapt SV. As seen in this thread where the BiPAP Auto SV has run into a brick wall.
Banned
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Sat Dec 12, 2009 4:14 am
by Muffy
Muffy wrote:Can you get a clear copy of the graphs from 2006?
CROWPAT wrote:I will try to get one.
I meant "readable".
However, for a good chunk of the night, sleep maintenance issues are again suggested:
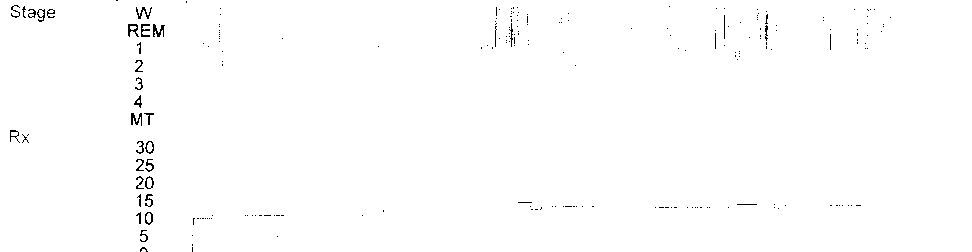
but try to get a "clean" copy of that.
Here's a challenge for -SWS. In that pile of data you have accumulated, find ANYTHING that says a pressure < 10cmH2O is DEFINITELY ineffective.
CROWPAT wrote:Got up, went out in 24 degrees, and walked for 30 minutes. Fog returned shortly after I got home, but no worse than usual.
Great. Repeat that 300 times.
While exercise has a number of great benefits, it has little value in weight control. You're probably going to have to cut your food intake by half (your requirement would be Daily Caloric Expenditure minus about 500 Calories to lose about a pound a week, which would be an excellent goal. Have 4 equally-divided meals).
There used to be a poster who blamed all the problems of the universe on GERD. A sleep architecture such as you've shown here deserves a look at that.
Muffy
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Sat Dec 12, 2009 6:52 am
by dsm
Guest wrote:timbalionguy wrote:So this begs a slightly off-topic but pertinent-to-the-discussion question: If one finds that they will have to use a servo ventilator, how does one go about making the right decision the first time? Or is this something that your clinician pretty much has to decide? These are really expensive machines, and very few can afford one of each.
The right decision the first time would default to the VPAP Adapt SV. As seen in this thread where the BiPAP Auto SV has run into a brick wall.
Banned
Banned so often I read one of your comments & am reminded of the boy who (Emperor`s new clothes) points us to some basic home truths.
Read thee as thee will
DSM
Nyuk, Nyuk, Nyuk!
Posted: Sat Dec 12, 2009 7:28 am
by Muffy
dsm wrote:Guest wrote:timbalionguy wrote:So this begs a slightly off-topic but pertinent-to-the-discussion question: If one finds that they will have to use a servo ventilator, how does one go about making the right decision the first time? Or is this something that your clinician pretty much has to decide? These are really expensive machines, and very few can afford one of each.
The right decision the first time would default to the VPAP Adapt SV. As seen in this thread where the BiPAP Auto SV has run into a brick wall.
Banned
Banned so often I read one of your comments & am reminded of the boy who (Emperor`s new clothes) points us to some basic home truths.
Read thee as thee will
DSM

Muffy
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Sat Dec 12, 2009 8:30 am
by -SWS
Muffy wrote:Here's a challenge for -SWS. In that pile of data you have accumulated, find ANYTHING that says a pressure < 10cmH2O is DEFINITELY ineffective.
You mean that well-known statistical 10cmH2O threshold in epidemiology? That very same 10cmH2O threshold beyond which
significant numbers of SDB patients begin to manifest central problems?
That same well-known 10cmH2O statistical threshold beyond which unnecessarily pressure-aggressive titrations can actually create more SDB problems than solve?
CROWPAT, I bet I threw that word
"statistical" in there just enough times to pique your interest in Muffy's possibility of a pressure-aggressive titration being a plausible explanation for some of your sleep issues. Muffy, I'll go back and see if I can find a shred of evidence contrary to that hypothesis.
Banned, dsm-- we really have to get some of these made up for the Resmed and Respironics buffs:


Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Sat Dec 12, 2009 8:45 am
by CROWPAT
No evidence at all of GERD being a problem for me.
Have never used CPAP/APAP/SV at pressures as low as 10.
Side note that I have not mentioned previously: I only eat dinner normally. Probably no more than 10 lunches a year and fewer than that number of breakfasts per year. Got into this routine from lots of field time while on active duty without time to eat the other meals. On days when I have breakfast or lunch I do not notice any change in physical feeling of tiredness.
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Sat Dec 12, 2009 10:56 am
by Banned
Muffy wrote:
Trust Us. LOL!!
Banned
Re: BIPAP AUTO-SV SETTINGS HELP
Posted: Sat Dec 12, 2009 11:23 am
by Patrick A
Banned wrote:Muffy wrote:
Trust Us. LOL!!
Banned
Hey those guys look familiar