Re: Had UPPP, Do I Have To Get A New Doc, To Get Help With This?
Posted: Mon May 11, 2009 4:04 pm
A Forum For All Things CPAP
https://www.cpaptalk.com/

robertmarilyn wrote:You trying to teach Muffy a lesson for his/her rant about graphs?
In as much as this thread is going to get a lot more confusing before if gets much clearer (if at all), it would be best to simply refer to Muffy as "Muffy", "Muffmeister", "The Muffburger", "Muffenstein" or "TPFKATPFKAS" with "her" comments.-SWS wrote:Because SAG/Muffy is such a well-qualified clinician, I like to "sit tight" and simply follow along as he offers his typically sharp clinical analysis.
See, whenever I see "robertmarilyn", it's tough to visualize what she looks like.robertmarilyn wrote:You trying to teach Muffy a lesson for his/her rant about graphs?
Since we now have some data to view, it might be a good idea to present these links and thoughts:StillAnotherGuest wrote:"IMHO", its not the letters anyway. Letters are not required to say something intelligent nor a guarantee that what will be said won't be stupid.
to see if they are pertinent.-SWS wrote:In light of the observations above, and the CFS diagnosis that Jan received, I have some interesting supporting links and pathophysiologic conjecture about hyperactive cognition-based arousals possibly having some degree of interrelatedness in neurology between overlapping CFS pathology and that of CompSAS/CSDB. Also a comment about a possible neurological stimulus/response mechanism that just may exist as an interrelated cohort for this particular hypothetical patient phenotype in neurology.
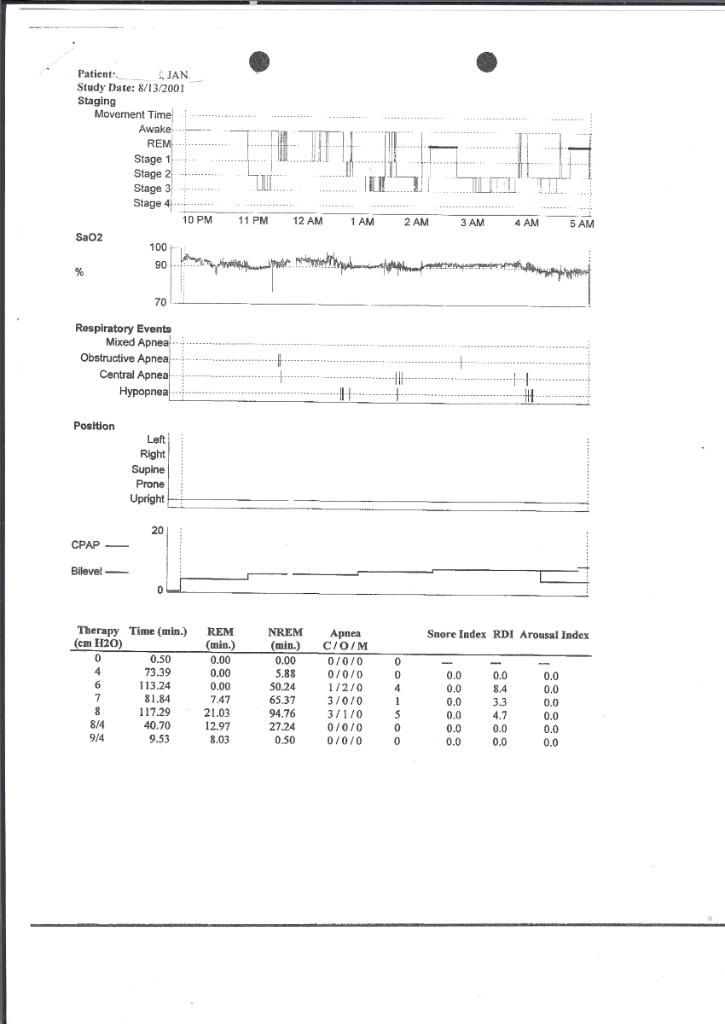
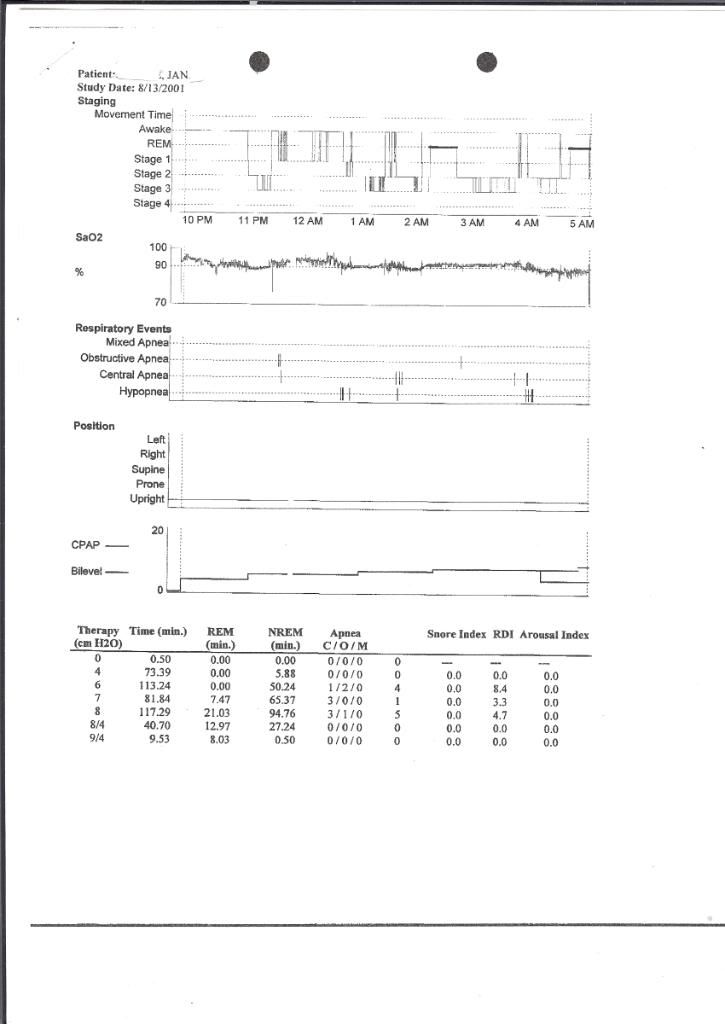
The Oxygen Saturation axis there is screwy (the 70% to 100% lines, are they 5% or 10% thresholds, I think they're 10s, back to that later). There seems to be a heavy supine dependency.12.08.2008 Report wrote:Pt was not split due to the amount of (night technician perceived) events seen throughout the night.
Starting out with 3.0 mg of Mirapex is pretty aggressive.Muffy wrote:but theSaltLakeJan wrote:My sleep tests were in May 2000,I have a list of the prescriptions I took for FMS/CF 3-2000 to 9-2000
Clonazapam 0.5 mg For Insomnia
Neurontin 300 mg Ambien 5 mg
Prilosec 20 mg Trazadone 100 mg
Effexor 75 mg
And based on that you went on 3.0 mg of Mirapex? What was the rationale for starting Mirapex and when did you start it?NPSG 3/3/00 wrote: LEG MOVEMENTS: Patient was noted to have 62 leg movements per hr of sleep. Most were associated with respiratory arousals.
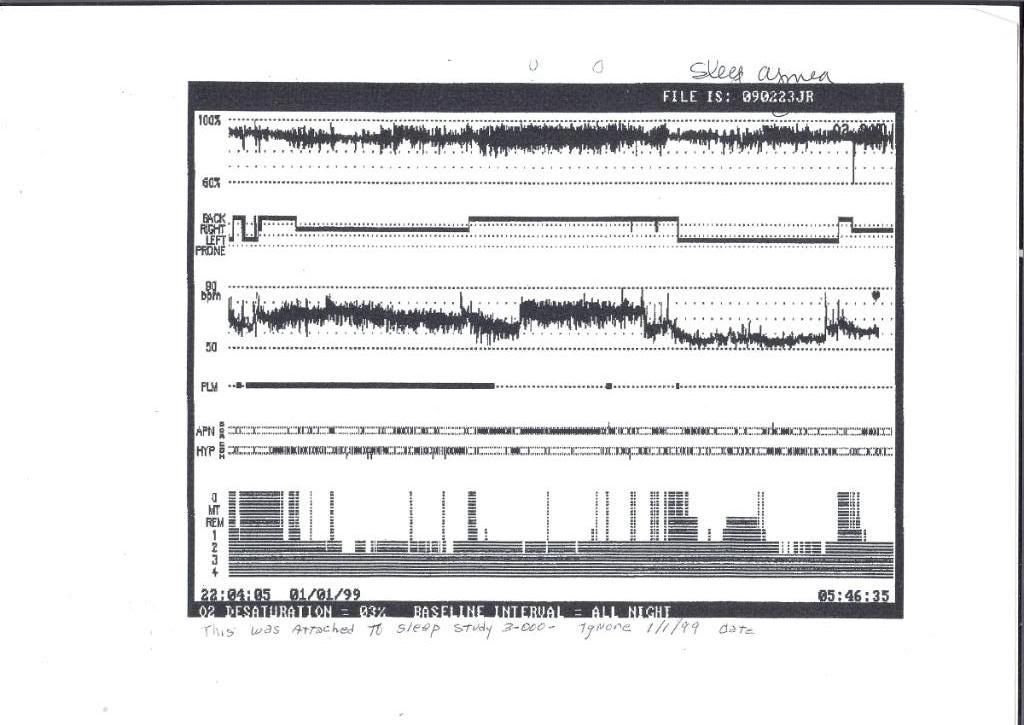
and then includes an epoch of SWS with alpha intrusion.12.8.2008 wrote:Technologist Comments: Pt a baseline study, no alpha intrusion
That's Muffin' to write home about (The Person Formerly Known As The Person Formerly Known As SAG)!Muffy wrote:Prologue
In as much as this thread is going to get a lot more confusing before if gets much clearer (if at all), it would be best to simply refer to Muffy as "Muffy", "Muffmeister", "The Muffburger", "Muffenstein" or "TPFKATPFKAS" with "her" comments.-SWS wrote:Because SAG/Muffy is such a well-qualified clinician, I like to "sit tight" and simply follow along as he offers his typically sharp clinical analysis.
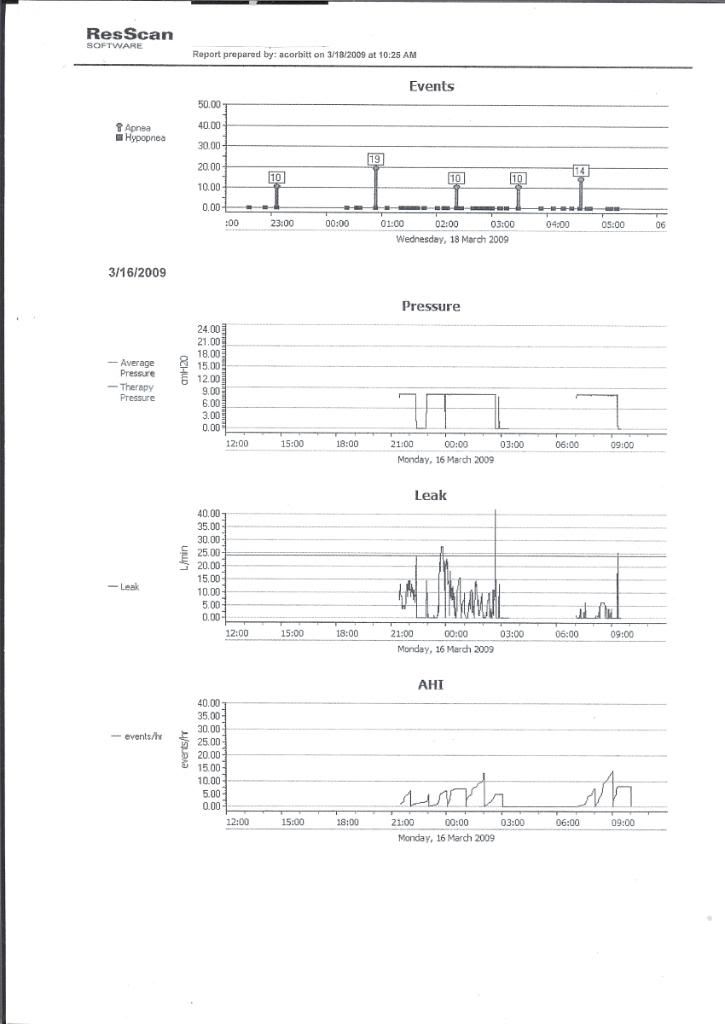
I'm thinking that while some charts will clearly be inconclusive, there will be salient clues to pick out and explore. Two patterned traits that I just so happen to tentatively have my eye peeled for are: 1) temporal characteristics of atypical cognitive and CNS variability (that can longitudinally manifest as atypical CNS variability), and 2) a possibly heightened cognitive arousability trait, that can be impacted by a variety of environmental, physiological, and psychological stimuli.Muffy wrote:However, in response to that point, each of these graphs is a summary or 900 pages of data, so even they may not give the true picture, and in some areas, I don't believe they do.robertmarilyn wrote:You trying to teach Muffy a lesson for his/her rant about graphs?
I think we're going to need the heart rate graphs (not the text) from the two most recent studies (2001 and 2008) in order to consider that approach and try to glean out HRV data, demonstrate that SLJ indeed has CFS or FBM, and somehow account for medication effect.-SWS wrote:Anyway, I have a working theory that some people presenting heightened-arousibility traits in cognition will often present: 1) more extreme CNS variability than most people, 2) more wake-to-stage-one sleep transition problems than most people (including insomnia), and 3) perhaps even a greater tendency toward CompSAS/CSDB maladaptation when presented with CPAP stimuli intended to resolve concomitant sleep apnea.
One Very Interesting Chronic Fatigue Syndrome Theory
Regard the Chronic Fatigue Syndrome, I have had overwhelming fatigue for years, When I think about it, I have to pesume you can have as many or few symptoms with it , as you have. Re: hyperactive cognition, would that relate to insomnia? When I used to go to bed, so many interesting ideas would occur, that I liked to stay awake and let a thought develop. However, since starting Cpap, the sensation of pressured breathing has kinda a hyponotic effect. It still takes a while for me to fall asleep. That may be long term habitual behavior. I have less than a month before my sleep study. I am starting an earlier bed time, perhaps this will help me get a longer sleep time in the study. I can't find the words I want to use to thank you, for the time you are spending on the search to discover the source of my problems. JanMuffy wrote:-SWS wrote:
In light of the observations above, and the CFS diagnosis that Jan received, I have some interesting supporting links and pathophysiologic conjecture about hyperactive cognition-based arousals possibly having some degree of interrelatedness in neurology between overlapping CFS pathology and that of CompSAS/CSDB. Also a comment about a possible neurological stimulus/response mechanism that just may exist as an interrelated cohort for this particular hypothetical patient phenotype in neurology.