OutaSync wrote:Well, if the Auto is giving me good treatment, then I would have give it up altogether, as I feel no better using it than I did using nothing. Why in the world would I want to tape and strap up the rest of my life just so that I can have more disturbances in my sleep than before?
I've put 14 months of my life into making this work, but you all have convinced me that it isn't going to get any better, no matter what machine I use. This is as good as it gets. Thanks, all...I'll take it from here.
Bev
I was going to ask you that,
how do you feel with no therapy at all?
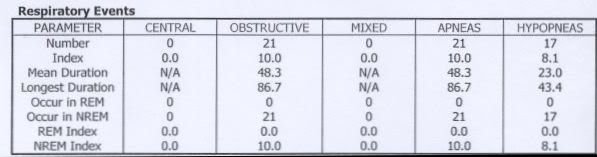
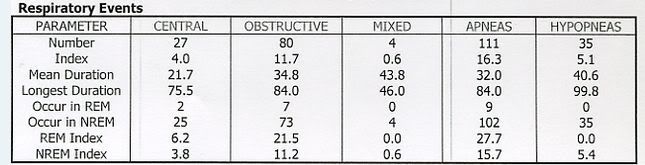
The thing dangerous about doing that is your oxygen levels drop dangerously low from the PSG from the very long duration of events seen. You cannot allow that to continue. While you don't feel any better due to daytime fatigue the lack of oxygen will destroy
your organs and create even more problems. Lack of memory is one indicator that is happening.
You must stay on a machine or go with supplemental oxygen.
I still think they missed your titration.
My suggestions:
1. I would put the SV back on auction, obviously it is no panacea in your case. If SAG said he didn't see any microarousals possibly
contributing to the daytime fatigue then the SV isn't going to help.
2. I would invest in a decent pulse oximeter like the CMS-50 and software (I can tell you how to install the software on Vista in Windows compatible mode).
3.
AFLEX: Put it in CPAP mode w/Cflex at 9.0 cm pressure. While you would still get data, you have to assume what you are looking
at is central events and the machine shouldn't be responding anyway.
You had ZERO events on the SV in CPAP mode.
4. Get a Sandman Auto and software (when you sell your other equipment). I'd sell the SV first, get a Sandman Auto with proceeds, sell the Aflex when you can as it is no better for you than the SV was (well a little better but it is the result that counts).
5. Address any allergies (even if you don't think you have any), most of us do.
Allergies: IF you have allergies and are taking something for it, maybe you need to shift when you take them? Such as taking them before bed as opposed to in the morning. Most allergy medications make you drowsy, in fact that is how many of the sleep medications were found to work, fatigue from adverse side effects when using them for allergies. I many times take Loratadine 10mg, before bed if I'm congested, it helps, they say it doesn't make you drowsy but they all do including Zyratec. I buy generic OTC AllerClear at Costco for $15 bucks for 300 tablets, its the same chemical makeup as Claritin only it costs way less. I would avoid the "D" or decongestant type it will overly dry you out, I
only use the antihistamine. Taking it also seems to help get past those sleep onset events. I have the same thing but mine is resolved using the machine, naps without the machine is another story.
6. I would see your doctor including your GP about a
trial on Provigil, hammer hard for it, you can read up on it below,
http://www.provigil.com/default.aspx
The Sandman Auto will do a couple things for you,
1. Address the obstructive aspect of your disorder from the full range of pressure.
2. Ignore any aspect of Central apnea seen, have the ability to record such activity including mixed events.
3. Allow you to use a lower pressure and help with complications from aerophagia.
4. IF other events are triggers such as FL runs you can fine tune this machine in how you want it to respond, with the
great details it gives in the reports that should be easy. Very easy machine to program.
5. Sandman will be much quieter at its lower pressure than even AFLEX. If the M series was quiet Respironics wouldn't have come out
with a noise silencer, they did that due to complaints of it being noisy. My 420e is quieter than my AFLEX. Higher the pressure the more
noisy they all are.