Snoredog wrote:I would like to see us discuss Inspiration Time and how that might change ones breathing to a particular scenario.
I think that's a good idea, Snoredog.
Snoredog wrote:Respironics keeps resorting to 1.2 seconds when it sees a problem, I wonder why they choose that value?
Well, Respironics is not telling clinicians to set IT at 1.2 seconds, as if that's a magic value. Rather Respironics is saying don't set IT at anything
less than 1.2 seconds if the titration-protocol decision branches happen to bring the clinician to that point. The sleep tech will set IT at the appropriate value based on measured respiratory parameters---
but no less than 1.2 seconds per Respironics' recommendation.
Again, that titration protocol is based on robust real-time measurements. And it's intended to occur in a single night. Short of being able to make those measurements, and differentiate central/obstructive/mixed events, etc. the suggested PSG titration procedures represent
FAR more bedroom guesswork than following Respironics' FAQ recommendation for this exact situation---at least as a starting point for Bev.
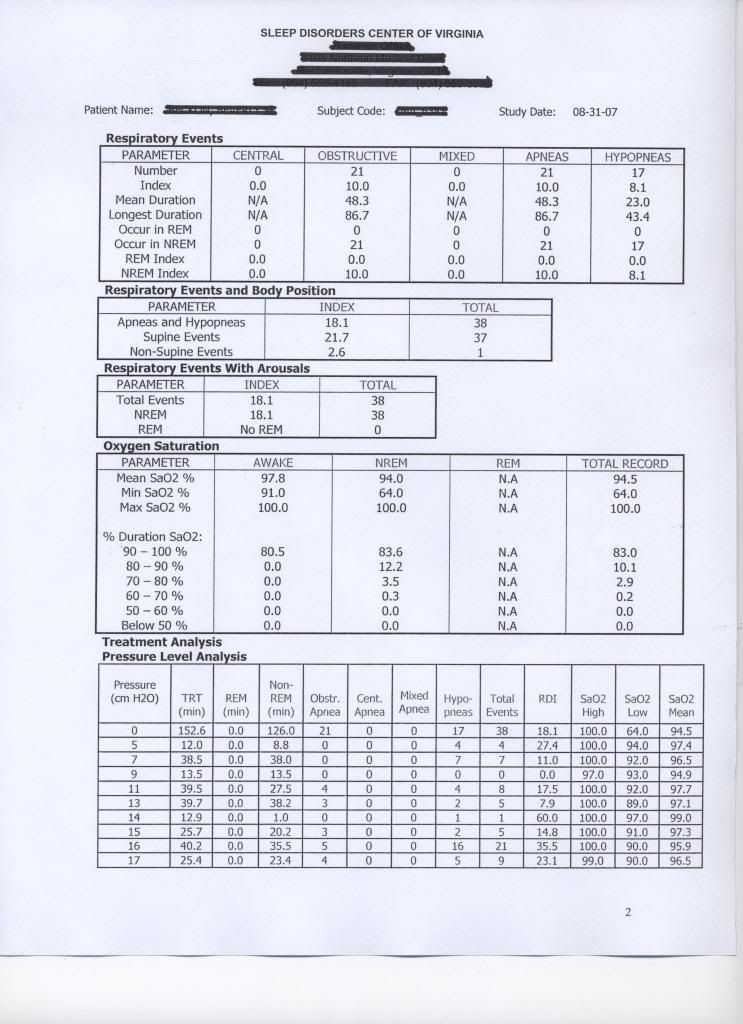
Starting with an EPAP of 14 cm, Bev should be able to replicate her current
very good AI and HI. IPAP max and Auto backup rate will work on any outstanding periodic breathing or central apneas. That's her best baseline from which to observe IPAP peak, IMO. Again, there shouldn't be much A or H at those settings based on her current results. She can unilaterally tweak down, 1 cm at a time, looking for improved comfort. As she does, she may need to extend IPAP max upward if that unilateral "tweak down" causes her to hit that diminishing IPAP max ceiling.
I agree there are always multiple ways to skin any cat. The FAQ suggestions are not just my preferred method, they are also the Respironics preferred method. How is Bev going to differentiate centrals and mixed events in her bedroom using a PSG titration protocol minus all that equipment? How is she going to determine which IT value (at no lower than 1.2) needs to be set?
Following the Respironics FAQ suggestion should really be a no brainer here. Attempting to perform a full-blown titration in the bedroom---with no PSG measurement and differentiation equipment---is admittedly more impressive for our egos. Bev's best sustained results are no less than 14. That's where her first night EPAP should be set IMO. And the other numbers should all key off that value exactly according to the Respironics FAQ recommendation. Overriding the Respironics suggestion for this situation, as if we somehow know more than the manufacturer does despite our limited experience, is also great for our egos.
I really think Respironics put their FAQ recommendations in place only after giving those procedures some very serious thought.
snoredog wrote:I see nothing wrong with following the lab titration guide, it teaches her on what to change to a particular condition instead of simply guessing.
But I do agree that the titration guide can provide help regarding what changes may be necessary when certain things go wrong---such as unresolved PB being scored on the Encore Charts.
Bifurcation is still a key clue with her IMO, but I won't go off on that tangent right now. More discussion on IT soon... for sure!
dsm wrote:I agree re using Respironics recomm titration - but, I would start Bev off at around 10 for epap as we already have a working baseline.
Doug, I missed that working baseline of 10 for epap. Where is that?