When probability fails....
Posted: Mon May 26, 2008 11:07 pm
One of the most impressive things in tangents' charts is the way her breathing cycles, runs and event correlate. When she snores, her cycles go all the way down, You can see it very clearly in her constant pressure chart.
When she runs she snores (...) and her cycles hit rock bottom.
Not so with me.

I rarely snore (on cpap).
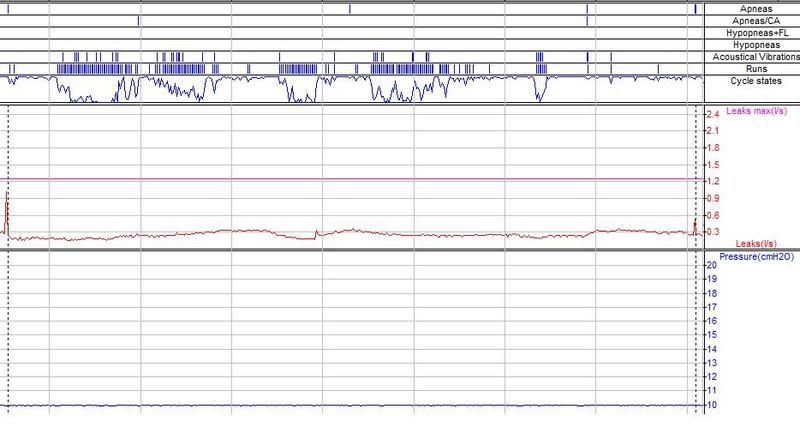
Many - maybe most of my events do not correlate with my cycle states - so much so that I stopped looking at that data and thought it was another bug. And the cycle state rarely reaches the bottom, if it does, it never stays there. This is true of both APAP and CPAP: I ran a min=max=my recommended for about a week last year - (it was disaster) and none of my events had much to do with either runs or cycles. Nothing looked like Cathy's up down.
Not so to with RG's data

In her recent min.= 7 experiment, she was snoring and having hypopneas, and her cycles were chugging along very near to top, obliviuosly - nothing like Cathy's cycles.
Not so with Bill's data
His cycles too have this fluctuating look most of the time (and hes' not snoring under therapy).
I suggest that anyone with that kind of constantly fluctuating cycle pattern needs IFL1 turned off, because the machine is getting false positive flow limitation runs on intermediate breaths, and is not capable of identifying whether pressure is needed or not.
And to return to Bill's original observation: Why do I have more runs when I cut the range? The answer is statisitics: The algorithm uses a Pearson correlation coefficient. When that statisitic has a more varied sample of breaths to work with, it gets a valid correlation. Correlation is lost (for mathematical reasons) when the variance drops. I'm not sure of the formal statistical term in English, in Hebrew that statistical phenomenon is called "cutting the range". Cutting the pressure range drops the breaths variance (for some of us) and we get wrong interpretations of our breathing patterns. Hence a built in option to turn IFL1 off.
O.
edited to add charts.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): CPAP, APAP
When she runs she snores (...) and her cycles hit rock bottom.
Not so with me.
I rarely snore (on cpap).
Many - maybe most of my events do not correlate with my cycle states - so much so that I stopped looking at that data and thought it was another bug. And the cycle state rarely reaches the bottom, if it does, it never stays there. This is true of both APAP and CPAP: I ran a min=max=my recommended for about a week last year - (it was disaster) and none of my events had much to do with either runs or cycles. Nothing looked like Cathy's up down.
Not so to with RG's data
In her recent min.= 7 experiment, she was snoring and having hypopneas, and her cycles were chugging along very near to top, obliviuosly - nothing like Cathy's cycles.
Not so with Bill's data
His cycles too have this fluctuating look most of the time (and hes' not snoring under therapy).
I suggest that anyone with that kind of constantly fluctuating cycle pattern needs IFL1 turned off, because the machine is getting false positive flow limitation runs on intermediate breaths, and is not capable of identifying whether pressure is needed or not.
And to return to Bill's original observation: Why do I have more runs when I cut the range? The answer is statisitics: The algorithm uses a Pearson correlation coefficient. When that statisitic has a more varied sample of breaths to work with, it gets a valid correlation. Correlation is lost (for mathematical reasons) when the variance drops. I'm not sure of the formal statistical term in English, in Hebrew that statistical phenomenon is called "cutting the range". Cutting the pressure range drops the breaths variance (for some of us) and we get wrong interpretations of our breathing patterns. Hence a built in option to turn IFL1 off.
O.
edited to add charts.
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): CPAP, APAP

