ozij wrote:Friends,
I've just lost almost 2 hours of work trying to compile something on this subject - due to a power failure.
pjwalman was worried about central apneas, had NR (non-resopnsive, therefore suspected central) apneas on a Respironics, and was loaned a PB by Rested Gal so she could see if that machine showed her having central apneas.
The first 2 nights settings ("setting no. 2"):
Peggy's first 2 nights on the PB420E had the following setting
Mode : Pilot : A+AV+IFL2
Min. pressure : 10.0 cmH2O
Initial pressure : 10.0 cmH2O
Max. pressure : 20.0 cmH2O
Max. press. for command on Apnea : 10.0 cmH2O
Ramp duration : 0 min

The results for the sessions when the machine was in use:
Events :
Index/h Apneas : 0.8
Index/h Apneas/CA : 0.6
Index/h Hypopneas : 3.1
Flow limited apneas Hypopneas: 0.5
Number Runs (FL): 230
Index/h Runs (FL): 53.1
And 53% flow limited breaths.
Each of 2 nights sessions had concentrated obstructive events, to which the machine responded sluggishly. There was no chance was those sustained obstructions could be healthy.


My reasoning was that Peggy has far more hyponeas than apneas (PSG and present data), IFL1 off really cuts response to hypopneas, so I suggested she turn IFL1 on and cap the pressure - with the amount of flow lmitation runs she had, I was afraid it would go stratospheric otherwise. I chose 14 because that's what seemed to stabilize her breathing on both nights. She was not having pressure induced apneas, and she was having (to my mind) unnecessary apneas.
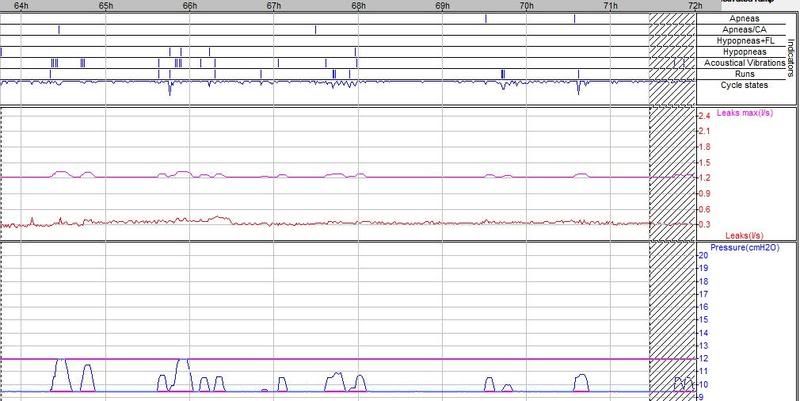
Compare the slow respond to the hypopnea buch in session 186 (alas, no snores to push the pressur along) to the fast rise on the first, where snores came along to help.
And note also, on session 187 how the machine does not respond to the apnea - because the maximum pressure for response on apnea was 10.
This it the next configuration:
Min. pressure : 10.0 cmH2O
Initial pressure : 11.0 cmH2O
Max. pressure : 14.0 cmH2O
Max. press. for command on Apnea : 12.0 cmH2O
The worst night for that period had an AHI of 4.9 - and the pressure hung at 14 most of the first night, it did drop, all the way to 10, and go back up agian, on the second night, which had 0 obstructive events, 0 hypopneas with flow limitation, a few snores and a few apneas/ca. Much better, and aerophagia was better too.
Clearly, those NR events on the Respironics were non responsive
obstructive events. We thought she may be dreaming at home, needing higher pressure, (1.5 mins of dreaming during the PSG) and maybe swallowing air during the struggle to breath.
The doc. was right about her central apneas being arousal responses.
I think that for some us, the PB mis-identifies flow limited cycles. As a result of that, it has far too many flow limitation runs and response to them pushes the pressure up too much.
On the other hand, when a person does have more hypopneic events, turning IFL1=off may mean they end up with a non responsive (or sluggish, to say the least) machine.
O.
Yep
use those settings should pretty much guarantee no response to anything but snore, it cannot respond to Apnea because the Maximum command on apnea is masked by the 10 cm Initial and Minimum pressure settings. If you uncheck any of the two IFLx boxes that will disable any response to FL either stand alone or combined with hypopnea.
I don't understand what one is trying to accomplish with use of those settings?
She can be assured that the "apnea/CA" seen on line 2 of session 183 are CA's with an open airway where cardiac oscillations were seen, that should be listed on the indice page.
I said when she had her Remstar and EncorePro reports that those "NR" events were Central, if you note the pressure she is at on the 420e in session 183 she is again at approximately 13cm pressure, SAME pressure where NR's showed up on her EncorePro reports on a totally different machine.
So how much more proof does one need?
She needs to LOWER her Initial & Minimum pressure to 8.0 and NOT mask off that Maximum "command on apnea" algorythm and ALLOW it to do its job. If the machine is responding TOO agressively to Flow Limitations (not hypopnea) she needs to turn IFL1 off. IF the machine continues to respond agressively remaining FL's associated with Hypopnea she then needs to "try" IFL2 unchecked.
If you shoot at the events seen with shot-gun settings you will never know exactly what parameter works and what doesn't. The conditions which aggrevate breathing and cause CA's to appear is agressive pressure, even constant CPAP pressure may cause them to appear.
She needs a machine that is smart enough to distinquish the difference between obstructive and central events, while the 42Oe is capable of doing that, you are circumventing it from doing that by use of those settings.
She should click on "Default" button under Settings and restore the machine back to default settings, then move Minimum and Initial pressure to 8.0. Leave command on apnea set at 10 cm. She should uncheck the IFL1 box so pressure returns faster to the Initial or Minimum setting sooner. Hanging on with pressure chasing FL's is not what you want when CA's are firing off, that only aggravates the condition.
You have to ask yourself WHY those CA's show up at 13 cm pressure and they don't at 10 cm? Yeah it hurts when I do that, then well don't do that.
Notice the CA just prior to therapy hour 89h, see the vertical dotted line in front of that indicating the "start" of a new session, that is a Sleep Onset CA, probably nothing you can do about that. But those events at hour 87.5 in session 183 are a train wreck.
The object of this game is to have a lower AHI and fewest events possible, that includes CA's and FL runs.
Having a 53% Flow Limited "session" is not my idea of very restfull sleep.
So far (excluding onset events), we know from her EncorePro reports that at 13-14 cm pressure CA's start showing up either as NR on the Remstar or CA on the 420e, nothing there has changed. So how did the 420e respond to those events in session 183?
Note: The machine does appear to increase pressure in session 183 after your red circle, and where you show it blown up with paint, notice the Apnea on line 1 and Central Apnea on line 2 "align" with each other, I would interpret that to be a "mixed" apnea and a break and another one right after it (the train wreck I referred to).
The pressure can resolve the obstructive apnea but it cannot do anything with the central portion left over.
IF I had to guess I'd say she has CSDB based upon those mixed apnea seen and how she responds to CPAP pressure.
First thing I would try is a mask that retains more CO2, flush out or exhaust out too much CO2 and the body's only response it can take is to stop breathing so it retains more CO2. Trying to fight that body response with conventional autopap may be frutile.
She would be better off using a lower pressure and allowing those Apnea that show up show up. This concept of setting pressure up like CPAP ain't gonna work with her condition cause CPAP won't work either, that is why they call it complex.
But I guarantee you if the machine is set up as I suggested and she used a Soyala mask that retains more CO2 she will see the best AHI she's ever seen and sleep like a baby.
Central apnea is a natural body response, if you manipulate breathing with a mechanical device in an adverse way it will adversely respond. In her case too much CO2 is being washed out so the body does the only thing it can that is stop breathing. If she is a shallow breather you are only spinning your wheels trying to address those Flow Limitations cause she's really breathing.
That's my opinion and I'm sticking to it, prove me wrong, I'd love to hear it