pjwalman wrote:So I think, Snoredog, that you are recommending I lower the maximum pressure to 11. And since I was having more events before when I had the lower pressures with the doc starting me at 6 (where I can hardly breathe, BTW), would a range of 8-11 be good do you think? Or could I even do a 9-11 or 10-11? I'd appreciate your input!
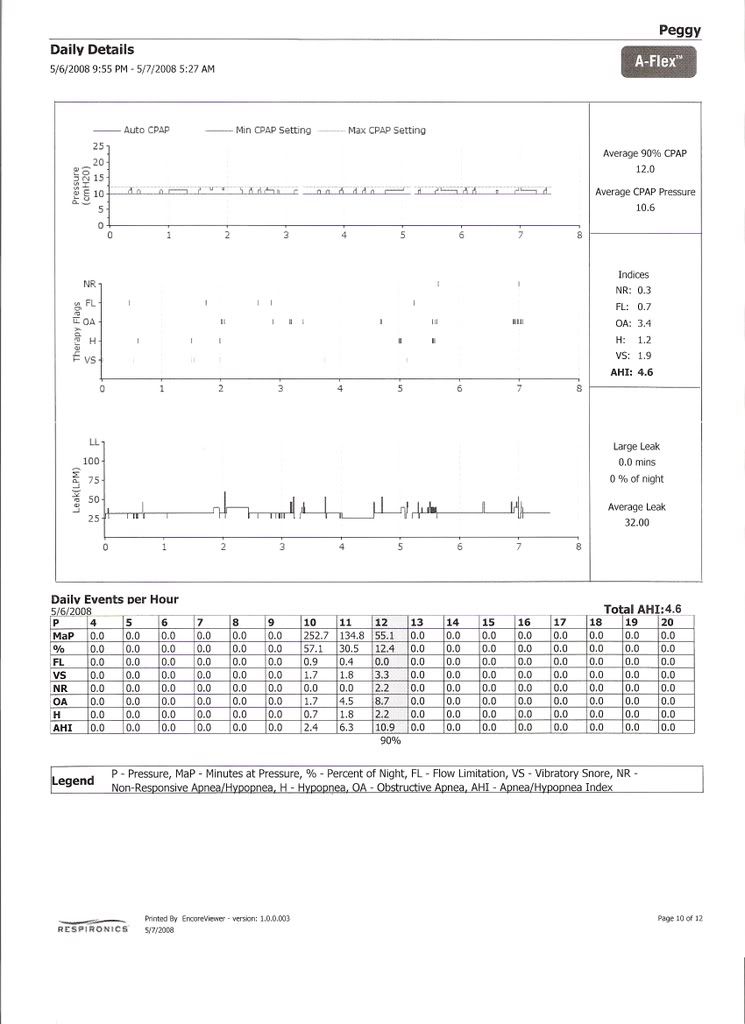
Peggy
NOTE: You NEED to forget the above "limit" settings suggestions when dealing with the 420e. Those suggestions were specific to the Remstar. Do NOT use them on your 420e.
I give suggestions based upon the machine you are using and how I know it functions algorithmically.
You cannot apply those principals on this different machine. The machine you had does a very poor job at differentiating the difference between a central apnea and obstructive. Some like to wing it and boast about that NRAH circuit but they are only fooling themselves. You no longer have that machine so forget those settings.
The 420e is a totally different animal, it will NOT respond to Central Apnea (CA) period. Remstar
responds to event first then asks questions later, the result is it makes lots of mistakes. By the time it realizes this it is too late it already responded with pressure, so you cannot turn back the clock you grow some balls throw up a flag and instead of saying you made a mistake you claim it as a feature.
But it is commonly known if you respond to a CA with pressure it will most likely get worse. That NRAH circuit on the Remstar can be compared to gee I hit myself in the head with the hammer 6 times and it still hurts think I'll stop now. So if you "know" that you start getting hit with the hammer at 13cm pressure you avoid that pressure by imposing limits, that was what was done on my prior pressure suggestion.
SO now you have a 420e, it doesn't respond like a Remstar, it responds similarly to a Resmed but even better. So the suggestions I make from now on will be geared towards your particular disorder and the current machine.
NOTE: There is NO reason to "limit" the pressure on a 420E. If it says it is a Central it will log it as such on line 2 of the 96 hour report, you can pretty much be assured if it says it is a CA that it won't be responding to it with increased pressure, it will either maintain current pressure or drop but it certainly won't increase pressure.
Now, what you have is a form of obstructive apnea combined with a few centrals. Is it CSDB? I would say not, but it means you need a machine that better responds more accurately to the event seen and does NOT respond to events where same pressure makes the event worse. You may need 14 or 15 cm pressure at certain times and it may not fire off a CA at all. Other times they may start firing off at 8.0 cm pressure.
Basically, you need a machine like the 420e that does a better job at differentiating the difference between a central and obstructive event. You want it to "respond" to obstructive events seen and "avoid" any response to Central Apnea seen.
However, the 420e was designed to function with a wide variety of patient needs and the default settings of the machine reflect that.
Based upon the events seen in your case (CA patterns seen), you may need to "tweak" the 420e so it better responds and/or more precisely to your particular need.
Minimum or Initial pressure:
You always want the machine
watching for events and NOT blindly responding to them like what happens when you use CPAP pressure or use a Minimum pressure set up "high". Toss out that set Minimum to CPAP titration theory as it does nothing in your case. You have CA at all different pressures, worst thing you can do is "hinder" the machine in early detection of those pre-curser events by using a Minimum pressure set up too high. For the first few weeks, have some faith in that little machine, it does a fine job if you allow it to.
Based upon what I seen above from the 420e data, you need to:
1. Increase the Max to 20 cm, there is absolutely no reason to be limiting the max pressure on the 420e.
2. Lower (yes I said lower) the Initial pressure from 11 down to 8.0. Allow the A10 parameter to work. If you have insomnia or cannot get to sleep due to machine noise/pressure etc. then set up the Ramp with even a lower pressure but no lower than 6.5. Use this during those nights you may awaken and find pressure to be annoying. Set the timer for 30 minutes.
3. Disable IFL1: This is "Command on Flow Limitation" setting, enabled the machine is aggressively responds to Flow Limitation. In your case you don't want that happening, you only want it responding to FL when it is associated with a Hypopnea (handled by IFL2 setting, leave that one checked).
4. After disabling by unchecking the IFL1 box, compare your reports, you should see the pressure sine wave change, it should have more sharp peaks and valleys compared to stairs or rolling hills. This means if the machine sees an apnea it will increase pressure to eliminate it, then drop back down faster so said pressure doesn't aggravate the condition that leads to more CA's. Your goal is to have NO CA's during the night. With a few tweaks on the machine you should be able to achieve that.
5. IF the CA's do not reduce then you may have to change the default pressure the machine uses to avoid response to CA when it cannot determine if an open airway exists. This is called "Command on Anea" or A10 parameter. By default it is set to 10 cm pressure. In your case you may need to lower it (never increase it), because your threshold for CA appearing may be lower than the industry standard of 10 cm pressure, we are human beings so you may not follow the status quo for that standard. If the CA's don't start lowering with the above settings you would slide the A10 parameter from current 10 to 9 and observe a few nights reports. Again, you are trying to stablize sleep so CA's return to zero. In its CA detection, the 420e listens for an open airway which allows it to hear your cardiac oscillations, kind goes back to the 2 cans and string theory from when we were kids. Those cardiac oscillations heard from an "open" airway is how the 420e it determines if the event is central or not. The Remstar and the Resmed don't do that or at least they don't advertise they do that. Remstar relies on that NRAH circuit and Resmed its patented A10. Now, not all CA's have an open airway (only about 60% do), the others may be closed, in the case of a closed airway, the 420e uses that A10 parameter to decide if it should respond with pressure (by having your Minimum set to 11 you are effectively "masking" that parameter OUT or disabling it where it does NOT function, reason to lower your Initial pressure back to 8.0).
If there is anyone that is conservative with machine pressure settings it is me, but don't hinder the machine from making decisions on its own by use of incorrect settings or following bad advise meant for CPAP.
IF you have plain jane run of the mill obstructive sleep apnea you can set it up like a cpap machine and get by with doing that. But you don't have run of the mill OSA it is complicated by centrals so it requires a bit more care in machine selection and setting it up correctly so it responds to your particular needs.
So based upon what I have seen, I would set your 420e up as follows:
Minimum pressure=8.0
Initial pressure=8.0
Max pressure=20
A10=10 (default command on Apnea setting)
IFL1=Disabled (unchecked, default=checked)
IFL2=Enabled (checked, default=checked)
IF CA's persist on line 2 after you set to above, you may need to lower A10 from current default 10 cm to 9.0 cm, this changes the way the machine responds based upon current delivery pressure. Basically it forces machine to watch for CA's at a lower pressure threshold when Cardiac Oscillations from an open airway are NOT seen indicating the event may be obstructive. This parameter is only used when no cardiac oscillation can be heard. So it says if current pressure is 10 or below and no cardiac oscillations are heard, apply pressure as the event is obstructive. If current pressure is OVER A10 or 10 cm and no cardiac oscillation are heard then it won't respond to the apnea for fear it may be central possibly with a closed airway such as with a mixed apnea, then it looks at pre-curser events like snoring to help decide if it should increase pressure or remain.
Low pressure can be your friend use it.