Posted: Thu Nov 15, 2007 7:37 am
Tolja.... Fat ticks cause even more Lyme disease.
O.
O.
LOL! Yes, you did!ozij wrote:Tolja.... Fat ticks cause even more Lyme disease.
O.
Hey there, O!ozij wrote:Hi there, -SWS!
Okay. Not to confuse data sampling rate (which occurs at the same rate in both machines) with graphical reporting. In general sampling rate potentially skews the specificity or sensitivity of instrumentation, but clinician's graphical reporting alone cannot. But reporting software can be highly erroneous as we all know.ozij wrote: I was thinking of that too - and when they changed from a 30 second sampling (418P) to a 60 second sample (420E)- it became an even rougher guide. But again, I agree - extremely helpful.
I think you've missed my points about the caveats of processing acoustic signals (those caveats are not relevant to the low-velocity signals). Please note the quoted patent text I have underlined above. I think that's where your signal-processing oversight lies. At that point in analyzing the patent text we need to back up and ask ourselves if we have nicely preserved or inadvertently deteriorated the acoustic signal (cardiac oscillations here).SAG wrote:What this suggests to me is that if 420E sees an event, and that event has respiratory frequency-based waveform activity that is <10% of the previous 2 minute analysis window, and the event is at least 10 seconds long plus five-eighths of the average of the preceding three breaths, and then it finds cardiac frequency (40-120 cycles/minute) waveform activity, then it will call that an ApneaCA. Consequently, the speed of waveform transmission becomes academic.
The above is from the patent. Now, I never studied physics in English, and what physics I studied was long ago. So I may be all wrong. But the way I understand this is that the amplitude of the flow is oscillating at the rate of human heartbeat - defined by PB as 40-120.the pressure waveform is examined for cardiac oscillation at step 76, i.e. regular, small-amplitude flow pulsations with a frequency in the range of the cardiac frequency
Signal amplitude speaks of the height/magnitude of the signal. Amplitude directly corresponds to how strong or faint the signal is. Frequency, of course, refers to cyclic repetition over time. Both parameters--amplitude and frequency--are essential to correctly processing this signal. When you see the patent text refer to a "small amplitude" flow pulsation, they are essentially saying that this signal is a relatively faint acoustic signal. That low signal amplitude, of course, makes the signal harder to baseline and subsequently measure/score when you generate signal reflection by mismatching acoustic impedances (the sensor's acoustic impedance versus the signal line's characteristic acoustic impedance in this case).ozij wrote:The above is from the patent. Now, I never studied physics in English, and what physics I studied was long ago. So I may be all wrong. But the way I understand this is that the amplitude of the flow is oscillating at the rate of human heartbeat - defined by PB as 40-120.the pressure waveform is examined for cardiac oscillation at step 76, i.e. regular, small-amplitude flow pulsations with a frequency in the range of the cardiac frequency
I cannot be sure, since we don't know the characteristic acoustic impedance of either tube. But if the argyle tube had a significantly different characteristic acoustic impedance compared to the original sensor line... then, indeed, the cardiac oscillation signal would have been amplitude-skewed (diminished during an ongoing baselining process) as well as being physically present on the signal line when it shouldn't have (as a faint signal echo during obstructive apneas---resulting in those false positives for central apneas).Ozij wrote: Do you mean, -SWS, that the info about this amplitude oscillation was affected by the Argyle tube ?
Right. That is not at all "front-end" data sampling. Front-end data sampling largely affects sensitivity, specificity, and even treatment (other issues do as well). Rather, what you see described here a a back-end process of finally getting around to reporting past-results to the clinician's software. That latter back-end reporting process doesn't impact the machine's detection or treatment algorithms regarding sensitivity or specificity.OziJ wrote: Re the sampling:
Silverlining's 420e manual says of the "detailed record": This screen analyzes the last 96 hours of operation including the recording of pressure (every 60 seconds).
Yes, that it clear to me, detection and therapy can be independent of the reporting.Right. That is not at all "front-end" data sampling. Front-end data sampling largely affects sensitivity, specificity, and even treatment (other issues do as well). Rather, what you see described here a a back-end process of finally getting around to reporting past-results to the clinician's software. That latter back-end reporting process doesn't impact the machine's detection or treatment algorithms regarding sensitivity or specificity.OziJ wrote:
Re the sampling:
Silverlining's 420e manual says of the "detailed record": This screen analyzes the last 96 hours of operation including the recording of pressure (every 60 seconds).
You mean this one?ozij wrote:If its not too much trouble, can you export that *.pat file you have for CLFDS (aka RG) to ascii, and then take a look at the *.SE file at the relevant session to see how may hypopneas are reported?
Code: Select all
File : C:\SL3\Patient\Oct19-2005StudyNight.pat
Start date : 10/19/2005
End date : 10/19/2005
Period : 1days
Used pressures (Average) :
Average pressure : 9.0 cmH2O
Low pressure : 8.0 cmH2O
High pressure : 11.0 cmH2O
Pressure efficient more than 90% of time :10.0 cmH2O
Events :
Number Apneas : 4
Index/h Apneas : 0.6
Number Apneas/CA : 14
Index/h Apneas/CA : 2.1
Number Hypopneas : 36
Index/h Hypopneas : 5.5
Number Acoustical Vib. : 22
Index/h Acoustical Vib. : 3.4
Number Runs (FL): 151
Index/h Runs (FL): 23.1
Cycle states :
Normal cycle : 80 %
Intermediate cycle : 2 %
Flow Limited cycle : 17 %
Invalid cycle : 1 %
Last settings of the period :
( 0 setting change )
Mode : Pilot : A+AV+IFL2
Min. pressure : 8.0 cmH2O
Initial pressure : 8.0 cmH2O
Max. pressure : 14.0 cmH2O
Max. press. for command on Apnea : 10.0 cmH2O
Ramp duration : 0 min

I had originally considered the possibility of the Argyle bubble contaminating the waveform when the events were first presented and tested that theory with a really outlandish length of bubble tubing pitted against a short length of standard 420E tubing, and there was no discernible difference:-SWS wrote:At that point in analyzing the patent text we need to back up and ask ourselves if we have nicely preserved or inadvertently deteriorated the acoustic signal (cardiac oscillations here).
Okay. I never followed this story too closely until now. I just took a very quick peek at your TAS post. Up until now I thought there was an issue with the 420e scoring central-apnea false-positives that Laura's same-night PSG did not score.SAG wrote:...yet the 420E events as scored are absolutely in keeping with the events in the PSG.
No events measured... or no pressure combined with no events measured?SAG wrote: I got another one where 420E misses EVERYTHING! And I mean everything!!
OK, I see that button.ozij wrote:No, I meant what you get when you export from the detailed record screen; That export creates 3 additional files (detailed data per session (*.se), detialed data per 24 hours, (*.24h) and a detailed leak and pressure summary for the last 96 hours (*.96h).
Hmmm. I'm gonna hafta import it to "Notepad", and separate it with an axe.ozij wrote:I import the files into Excel, the separator is a semi colon.
How can that be, it looks like the same routine as the other report I sent you:ozij wrote:I thind the apnea and hypopnea details on the *.se file will be different from those we saw till now.
Code: Select all
File : C:\SL3\Patient\Oct19-2005StudyNight.pat
Start date : 10/19/2005
End date : 10/19/2005
Events :
Number Apneas : 4
Number Apneas/CA : 14
Number Hypopneas : 36
Code: Select all
File : C:\SL3\Patient\Oct19-2005StudyNight.SE
Apneas: 1
Apneas/CA: 14
Hypopneas: 36
In all fairness to APAP algorithms the world 'round, it might be more appropriate to call this a design "limitation". The point of this one and RG's is that if you're trying to do diagnostics with single-channel data acquisition, there is a percentage of patients where major underlying disease states will be missed.-SWS wrote:No events measured... or no pressure combined with no events measured?SAG wrote: I got another one where 420E misses EVERYTHING! And I mean everything!!
So far this one sounds like a malfunction versus design shortcoming.
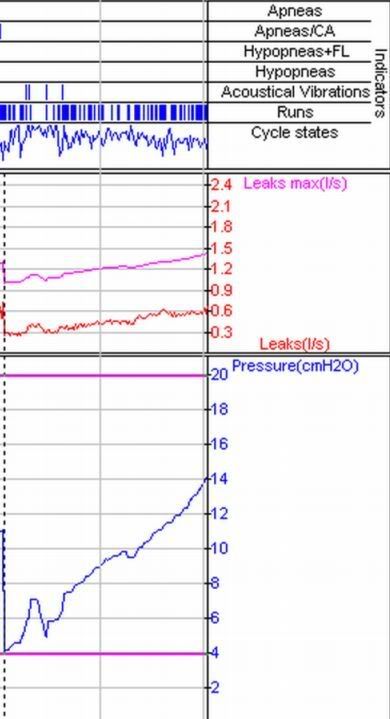
In the "this one" screenshot of a two hour session... the person using a range of 4 - 20. Was IFL1 on?StillAnotherGuest wrote:The point of this one and RG's is that if you're trying to do diagnostics with single-channel data acquisition, there is a percentage of patients where major underlying disease states will be missed.
Submitted for your approval-- one strange APAP response:
SAG