Posted: Fri Nov 09, 2007 8:52 am
I'd try Nexium. Or, at least OTC Prilosec.
I'd give 'em at least a week to see if either helped the situation.
I'd give 'em at least a week to see if either helped the situation.
Train wreck is based on the amount or frequency of the events seen on your EncorePro reports (lots of activity), it would be nice to see it settle down where fewer events were seen and that's how you know you have achieved ideal cpap therapy is when the number of events seen start dropping off. Increased pressure doesn't always eliminate those events.MRH wrote:Snoredog,
What do you mean by train wreck? My ahi is a fair amount lower then before and it must be because i slept on my side (Thank you for that advice) Last night was even a bit better ahi at 6 something. I figure I might give it a few more nights to see what happens now before I change things again. I have been doing a bunch of changing and am afraid I could end up just chasing myself around. I can see where that could happen real easy!
Ahh, the loonlvr story.rested gal wrote:hehehSnoredog wrote:And I ain't buying any stubborn GERD theories here either.]
Well, I am.
Looks an awful lot like what was happening with loonlvr a long time ago:
Mar 10, 2005 subject: What is the REMStar Auto really doing? Derek, -SWS, Wader, and a very intelligent "Fascinated" Guest discuss loonlvr's posted charts. Extremely interesting 5 page topic.
Mar 18, 2005 subject: What's REMStar Auto Really Doing? - new thread Derek posts more of loonlvr's charts.
Nov 05, 2005 subject: SUCCESS AT LAST-GERD,420E, PRILOSEC AND BENADRYL -SWS's thoughts on loonlvr's massive clusters of events and loonlvr's followup post.
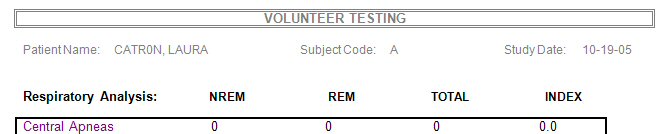
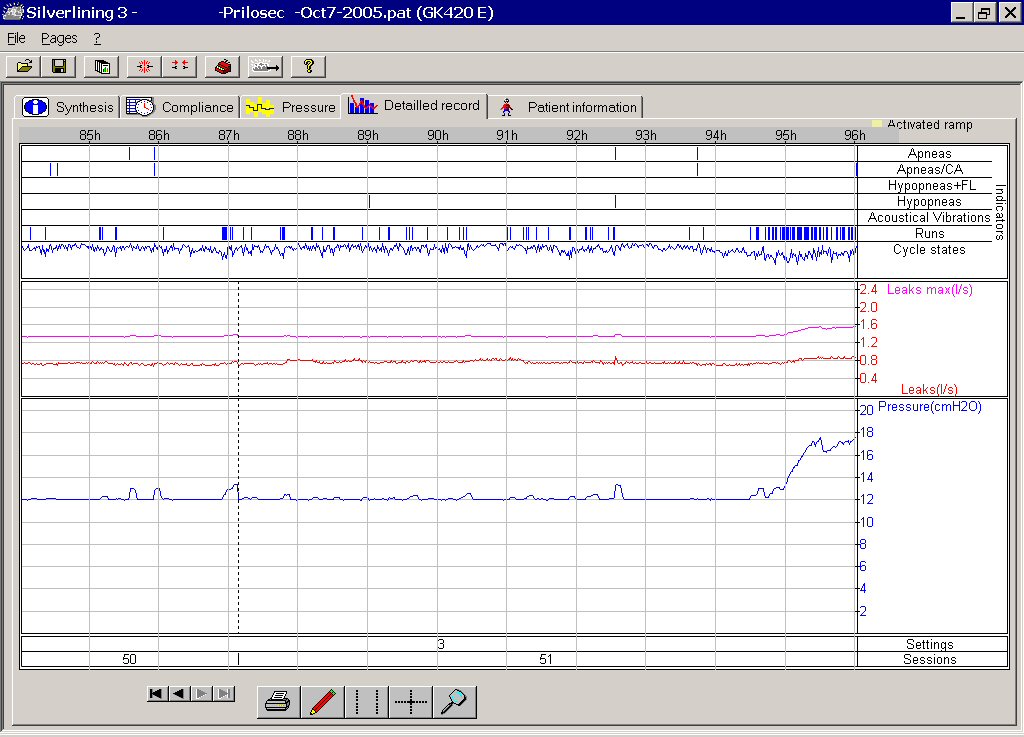
How's that again? There are very few central apneas on this "before " report - almost all the ones on the "Apenea/CA" line have an obstructive one on the line above - which means they do have obstructive involvement.StillAnotherGuest wrote:5. The behavior of the 420E (identifying mostly central apneas), if anything, suggests there that isn't obstructive involvement
I was struck by a strange and interesting thing when comparing theseLaura, I thought of another possibility to throw into
the mix after I sent you that email. Namely, vocal chord
spasms. Researchers believe that at least some apneas
and hypopneas may not involve the upper dilator muscles---
but rather are a function of the vocal chords themselves
experiencing spasms. Those who subscribe to this school
of thought attribute these vocal chord spasms to repeated
or ongoing exposure to stomach acid (among other possible
causes or physiological triggers such as stress).
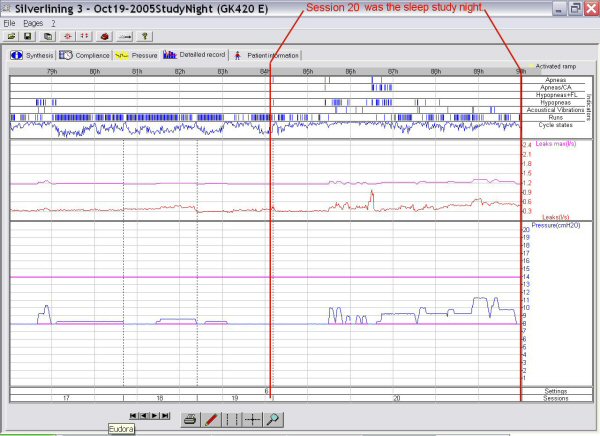
Looking at Mike's (somewhat atypical) "strings" or
clusters of SDB events I can't help but wonder if this
vocal-chord-based etiology doesn't fit his particular
pattern of events:
1) isolated episodes, as are typical of spasms in general.
2) unrelated to sleep stage, unlike typical upper airway
dilator muscle apneas. (Mike can have one-to-two hour
episodes, which outlast several sleep stages.)
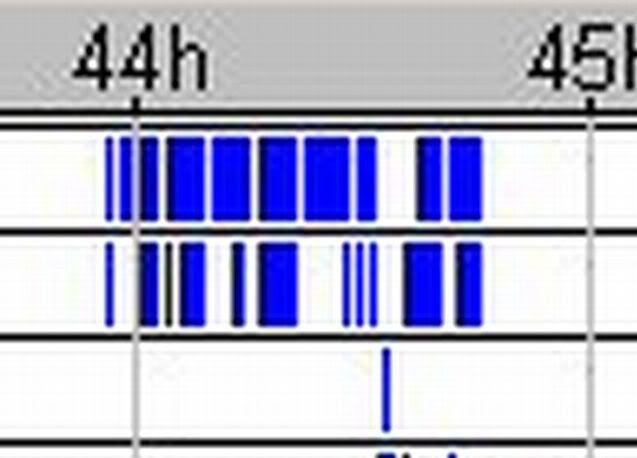
3) long strings of mixed events are sometimes shown on
Mike's SL3 reports---meaning sometimes his airway is
open enough to convey cardiac oscillations (as an
inefficient acoustical waveguide) and yet other times
there are no cardiac oscillations present (sometimes
there are even interspersed snores).
Yeah, the good old loonlvr story.StillAnotherGuest wrote:Ahh, the loonlvr story.
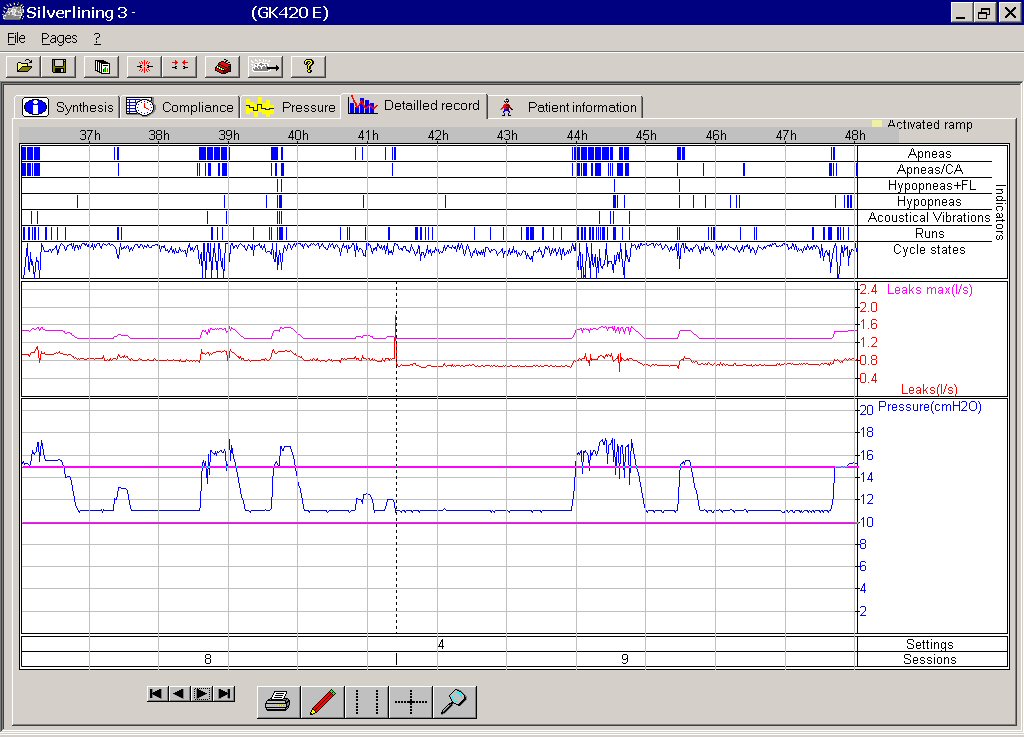
I agree, the software can't tell us that. But I think when pressure (and more pressure and more pressure) doesn't control events, that might sometimes be a clue to look a little more closely at the possibility of GERD interfering with how a cpap does its job...the job being to push aside soft tissue while we breathe.StillAnotherGuest wrote:I'd like to offer the following discussion points:
1. You can't tell anything about the existence or extent of GERD with PAP Software.
Yes, let's do forget about benadryl for a sec, and concentrate on Prilosec.StillAnotherGuest wrote:2. The use of benadryl in any capacity to affect sleep these days is darn near negligent. With a half life of about 9 hours (actually, who knows what it is in a given individual), if you take it at bedtime, or later, you could very well be driving to work in a grog.
3. If you do get into an accident, and the Officer says, "Here, we want you to pee into this container", reread #2. On second thought, forget it.
Hey, I'm forgetting about benadryl. Remember?StillAnotherGuest wrote:4. Any airway involvement that was severe enough to respond to benadryl would have a myriad of other symptoms, it certainly wouldn't be "silent".
Lost me there...?StillAnotherGuest wrote:5. The behavior of the 420E (identifying mostly central apneas), if anything, suggests there that isn't obstructive involvement.
loonlvr sent me the Silverlining .pat file. But that's long gone in a computer crash I had a year or so ago.ozij wrote:RG, did you only get the jpegs, or do you by any chance still have the original data files?
O.
SAG would speculate that if that's what was occurring, loonlvr's sleep efficiency would be about 25%.rested gal wrote:When the loonlvr mystery was unfolding, -SWS speculated that IF a person's esophagus was getting nightly acid baths from GERD, it could lead to irritated, inflamed tissue. Swollen tissue. Rigid tissue. Hard tissue that's more difficult for cpap air to push aside.
Actually, I think Benadryl made a critical contribution here, just not in the way you think.rested gal wrote:Yes, let's do forget about benadryl for a sec, and concentrate on Prilosec.
I think you can make a good case for that. But I don't think that what you think about what -SWS thinks about loonlvr is what I think you should be thinking. Ya think?rested gal wrote:Back to the Prilosec, which is what I think really did the trick for loonlvr.
I think I still think what I was thinking thanks to -SWS's thinking.StillAnotherGuest wrote:I think you can make a good case for that. But I don't think that what you think about what -SWS thinks about loonlvr is what I think you should be thinking. Ya think?rested gal wrote:Back to the Prilosec, which is what I think really did the trick for loonlvr.
SAG
Yep...I'm still chuckling.StillAnotherGuest in his catchy post title wrote:Didn't You Think Peeing in the Cup Was Funny?
Cause if you weren't busy raking, you could help me.ozij wrote:Yes, we got trees... why?
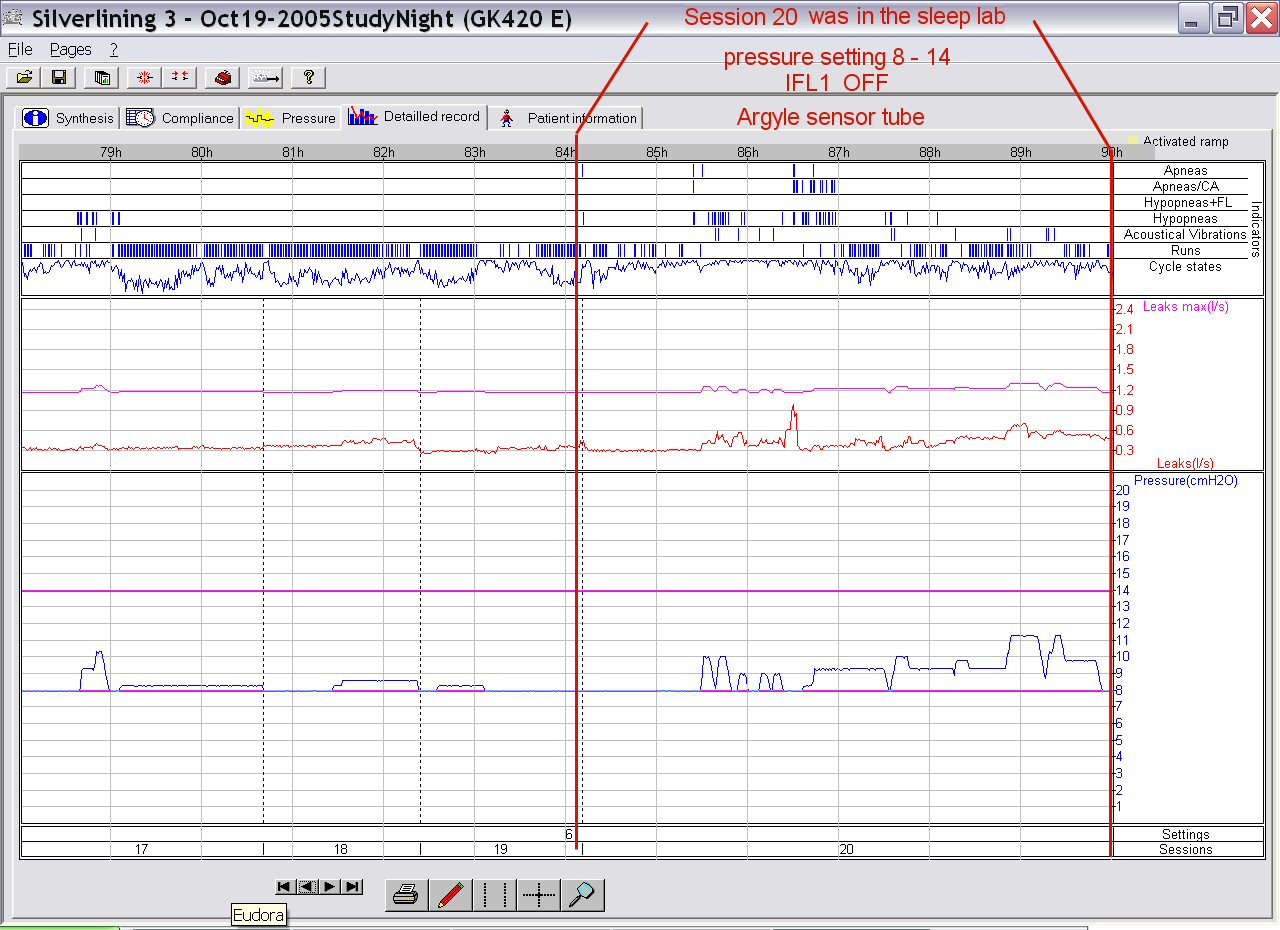
As I understand the concurrent ticks concept in SL3, it is not a "mixed apnea", rather, it is a "mixed acquisition of cardiac oscillation signals". The only way you could call it a mixed apnea is if SL3 was 100% accurate in identifying central apneas, which it's not. It's only 100% accurate (in a small study) in saying that the centrals it does find are centrals.ozij wrote:And why do you think that airway is wide open? I mean, how do you explain those apnea (non c/a) above the apnea non c/a marks?
I think you should think about what the role of the benadryl is here.ozij wrote:And, what is it you think we should think?
So, a "double tick apnea" is one which is central, but part of the time the machine is loosing the heartbeat and that's why it's adding the top tick?StillAnotherGuest wrote:As I understand the concurrent ticks concept in SL3, it is not a "mixed apnea", rather, it is a "mixed acquisition of cardiac oscillation signals". The only way you could call it a mixed apnea is if SL3 was 100% accurate in identifying central apneas, which it's not. It's only 100% accurate (in a small study) in saying that the centrals it does find are centrals
I've kept forgetting (for two years now!) to ask about something:StillAnotherGuest wrote:It's only 100% accurate (in a small study) in saying that the centrals it does find are centrals.
{kind=link}
{kind=link}
{kind=link}