StillAnotherGuest wrote: split_city wrote:Now, my understanding is that pleural pressure at FRC is negative because opposite forces acting on it (inwards recoil of lungs and outwards recoil of the chest) acts to pull the lungs from the chest wall. Correct?
Intrapleural pressure is normally always negative. When it isn't, the lung turns into a raisin.
At full expiration and during forced expiration such as the case during a spirometery test, intrapleural pressure becomes positive. This is why we still have air inside the lungs at RV because the postive pleural pressure compresses the airways, trapping air downstream.
StillAnotherGuest wrote: split_city wrote:After all this discussion, are you suggesting that my negative Pes @ FRC readings are incorrect??
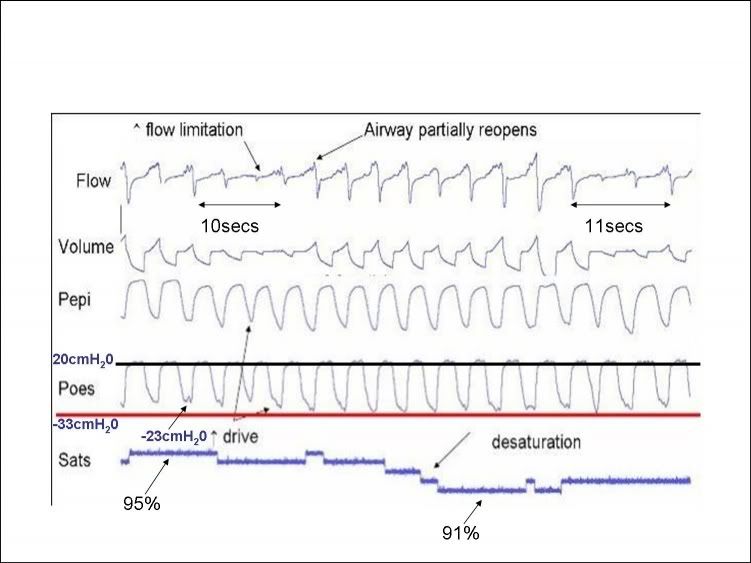
No, the +20 cmH2O seen during exhalation during a period of baseline breathing.
I have already discussed the reasons why peak Pes is increased. You must remember, this +20cmH20 also includes the +5-10cmH20 artifact caused by the compression of the medialstinal structures. The true peak value is likely to be between 10-15cmH20. All the other patients also had increased peak expiratory Pes during their apneas. I'm pretty sure peak Pes also increased during hypopneas in other patients.
You keep saying baseline breathing. I keep disagreeing with this because the patient is under a high drive state. What would you call his breathing when his airway is patent and there is no flow limitation? Baseline, baseline breathing??
StillAnotherGuest wrote:
My point is that that value needs explanation. Either something has caused expiration to go from passive to active (although there's nothing there that would indicate that, like bronchospasm or upper airway obstruction) or the calibration is incorrect.
I told you why his expiration has become active. The patient is under a high drive state because his airway is acting as a Starling resistor. I have no doubt he was actively recruiting his abdominal muscles.
StillAnotherGuest wrote: split_city wrote:Pes is commonly used as a surrogate measure for pleural pressure. Given that pleural pressure is subatmospheric at FRC, Pes will also be negative. Correct? I have seen a number of papers stating that Pes is negative at FRC. Do you think Pes = intrapulmonary pressure?
Is this a trick question? Oh what the hey, I'll go with sure, as long as the patient has no disease that causes loss of compliance.
There are no smoke and mirrors. You have clearly stated that you believe that Pes should be zero at FRC.
StillAnotherGuest wrote:so baseline Pes is normally 0 cmH2O
StillAnotherGuest wrote:(and for that matter, Pes) are open to air, so if allowed to equilibrate, P will = 0
What the hey, I'll provide some references to show you that Pes is negative at FRC, thus confirming that Pes does not equal intrapulmonary pressure.
I have said that Pes can be used as an alternative measure for pleural pressure.
Here is a study comparing pleural pressure with Pes in humans
Mead et al (1959) Journal of Applied Physiology 14(1): 81-83
Upright
Mean pleural pressure at end-expiration was -5.1cmH20
Mean esophageal pressure at end-expiration was -4.8cmH20
Supine
Mean pleural pressure at end-expiration was -1.1cmH20
Mean esophageal pressure at end-expiration was +2.6cmH20
They did not mention the BMI of the subjects
Other studies which have shown Pes to be negative at end-expiration include:
Mead et al (1963) Journal of Applied Physiology 18(2): 295-296
Ferris et al (1959) Journal of Applied Physiology 14(4): 521-524
Coulam and Wood (1971) Journal of Applied Physiology 31(2): 277-287
Gillespie et al (1973) Journal of Applied Physiology 35(5): 709-713 showed that Pes correlated well with pleural pressure in the anesthetized dog.
I hope this clears it up for you.
Going back to the first point. Now remember, it has been shown that Pes is considered a relatively good alternative measurement of pleural pressure (in the upright posture anyway), Mead et al (1955), Knowles et al (1959) and Milic-Emili et al (1964) all showed that Pes was positive at RV
