Posted: Fri Mar 09, 2007 11:45 pm
Please see the responses to your other three threads sleepyjane.
You can take SAG's quotes and play them back over and over and they don't apply in every case. you guys seem to be bundling CSDB and central apnea in the same category which it is not. Central apnea can occur without any cpap machine in the picture at all, such as the case with myself and bluegrassfan, frequenseeker and many others I've seen come by here. With CSDB the apnea condition gets worse on cpap.rested gal wrote:Snoredog, you've done a lot of experimenting with a lot of machines while working on your own treatment. The type of sleep disordered breathing that showed up on your PSG happened to involve a lot of centrals for you. Your lab titration and your own use of autopaps found what's right for you. I don't know this for a fact, but my guess is that your case is rather unusual compared to the type of sleep disordered breathing most people have.
If that Mayo study is right, approximately 85% don't have the kind of SDB problem that may be what was revealed in your PSG sleep study, Snoredog...i.e. the numerous centrals you had along with your other OSA events. The experience you have when you increase pressure is not likely to happen to most people with plain OSA who choose to use an autopap, imho. I think your own experience very much colors your advice about autopap settings. But then, that's probably so to one extent or another for all of us.StillAnotherGuest wrote:Morgenthaler et al at Mayo in Complex Sleep Apnea Syndrome: Is It a Unique Clinical Syndrome? in SLEEP 2006:9 showed that the incidence of CompSAS (which would pretty much be the thing that would get you into trouble with pressure-induced events) was about 15%, so that might be a good number to start with.
SAG
I do think that your insistence on the danger of raising pressure and risking "pressure induced centrals" is overstating the possibility because you've seen that happen to you. I don't think that would happen to most people using autopap. Just my opinion, and I'm not a doctor.
viewtopic.php?t=14225
Page 2:(bold emphasis mine)StillAnotherGuest wrote:The phenomena of pressure-induced central apneas is tossed around far too freely. The vast majority of people do not get centrals because of ultra-therapeutic CPAP levels. BiLevel, Pressure Support (PSV) and Proportional Assist (PAV) Ventilation are another matter. You need some mechanism to drive the pCO2 below the sleeping apneic threshold, and plain old CPAP rarely is able to do that. OK, if you wanna argue that CPAP increases base lung volume (Functional Residual Capacity)(FRC), and since that increases gas exchange, some people can generate centrals that way, fine. But it's not as many as you might think.
SAG
True, SAG was referring to "plain old CPAP", not autopaps. However, I think autopaps are delivering one straight cpap pressure, too...varying that pressure, yes. But I think autopaps are more in the category of "CPAP" than being the type of machines that would deliver the kind of treatment (BiLevel, PSV, PAV) he goes on to speak of as being "another matter."
Although SAG generally prefers to play "Panama" by Van Halen repeatedly.Snoredog wrote:You can take SAG's quotes and play them back over and over
This is perhaps the most important point of the half dozen concepts here. Are you better, worse or the same. The large scale study of the effects of CPAP on CHF/CSA in CANPAP showed that CPAP actually dropped the AHI by half (40 to 21). Maybe not the best, but certainly better. And if you wanna say pressure therapy generates centrals, then there has to be a bunch, like a burst at an AHI rate of 40-60 because the cascade is set in motion and each central will force another. All these guys that go "Omigod, a central apnea, it's the apocalypse!!!" need to take some venlafaxine (no, no, don't do that, only kidding!!). The relationship of isolated CA during aggressive pressure titration is often as a result of arousal (high pressure aggravates patient, he then has arousal, briefly hyperventilates, has compensatory CA (which makes it a NORMAL response) and returns to baseline).you guys seem to be bundling CSDB and central apnea in the same category which it is not....With CSDB the apnea condition gets worse on cpap.
Right, but they claim 100% sensitivity for all apneas, so we can still get a clue.PB themselves admit that the 420e can only detect or differentiate central apnea 66% of the time even on a good day.
That ain't Wally. Wally's much taller...look at how many Apnea/CA's Wally had in that report above.
You would have been right.if I had to guess there is a apnea along with those CA's so some of those are probably Mixed apnea.
To illustrate that point, these guys noted that the number jumps to 28%:RG said that SAG said that SAG read... wrote:The phenomena of pressure-induced central apneas is tossed around far too freely. The vast majority of people do not get centrals because of ultra-therapeutic CPAP levels. BiLevel, Pressure Support (PSV) and Proportional Assist (PAV) Ventilation are another matter. You need some mechanism to drive the pCO2 below the sleeping apneic threshold, and plain old CPAP rarely is able to do that.
Right, that's the fine line. But you do have to address the snoring, and if it's generating arousals you are obligated to attack it. SAG shoots techs who leave residual snoring in titrations.Ask SAG what terminates a titration study. He'll tell you, when the obstructive events subside and good sleep is obtained. But if the patient snores, they may try to also eliminate those snores and in doing so they can cause a central which wakes the patient, from the pressure being too high.
The above APAP disaster was actually set up by some genius DME RT. Seems like I'm always fixing their botched mess of pseduo-medical trickery (pseduo?).Sure enough, they order it, it shows up plug it in leave it at default 4cm to 20cm range as set by some genius RT
Nonsense, SAG. Every time I see a SAG posting, I immediately jump to it. The combination of sage wisdom, humor, and detailed guidance you offer is as good as it gets on this forum. You serve as an inspiration for aspiration.StillAnotherGuest wrote:Perhaps SAG will post as "Black Bart" so he can fire off personal barbs, since he is unfortunately aware that the mudslinging threads get about 7 to 10 times more views than the more civil posts.
StillAnotherGuest wrote: Seems like I'm always fixing their botched mess of pseduo-medical trickery (pseduo?).
StillAnotherGuest wrote:It happens a great deal more than you think.
SAG
Well, yeah, I was, kinda. My first titration study I only slept 42 minutes the entire night.BrianRT wrote:ummmm......I 'THINK' it nevers happens in my dealings with sleep labs. IF it does, then GREAT, it SHOULD be the default, instead of the exception. My point is, a number of sleep labs use auto's as their 'go-to' device when they can't properly titrate (*gasp* dirty insider secret just leaked folks...no pun intended). Problem is, the patient has to pay for that 2nd night titration study when NOTHING WAS ACCOMPLISHED.
But, if it happens 'a great deal more than I think', then let me ask the opinions of the residents of this fine forum. Has anyone ever been told to come back for another titration study because the lab couldn't quite get it right the first time??
You keep implying that even some harmless, "normal" centrals mean DANGER!! And that the instant even one central shows up during the course of some peoples' sleep lab titrations, it's a big deal. Both christinequilts (who DOES have Central Sleep Apnea) and StillAnotherGuest (also as "sleepydave") have explained many times that there can be perfectly normal ways that central apneas can happen -- asleep or awake. Even in perfectly normal people that have no OSA or any kind of sleep disordered breathing at all.Snoredog wrote:Take 100 patients, put them in a lab titration setting, use SAG or anyone you want, start titrating them from 5cm and continue to increase to 20cm then count up the number of patients that blew CA's, I'll bet you there are a lot more than just 15 out of those 100. Your diagnostic PSG can show 0 (zero) CA's then when you apply cpap pressure they can show up (or not show up).
(bold emphasis mine)StillAnotherGuest wrote:All these guys that go "Omigod, a central apnea, it's the apocalypse!!!" need to take some venlafaxine (no, no, don't do that, only kidding!!). The relationship of isolated CA during aggressive pressure titration is often as a result of arousal (high pressure aggravates patient, he then has arousal, briefly hyperventilates, has compensatory CA (which makes it a NORMAL response) and returns to baseline).
Just checking to see how the consensus is shaping up...On the Subject of APAPs CollegeGirl wrote: I think we need to at least try to come to some sort of general consensus on things... (If that's even possible).
If you're referring to the PB420E graph on page 2, I still wish I could'a sneaked in there to flip off IFL1.StillAnotherGuest wrote:The above APAP disaster
Yeah I thought that was Wally's reports also, my bad. But in your reports, there is a HUGE improvement in the lower chart.rested gal wrote:If you're referring to the PB420E graph on page 2, I still wish I could'a sneaked in there to flip off IFL1.StillAnotherGuest wrote:The above APAP disaster
Might not have made one bit of difference for Wally. Oh, wait, you said that wasn't Wally??? I could have sworn the peaks looked tall enough to be him!
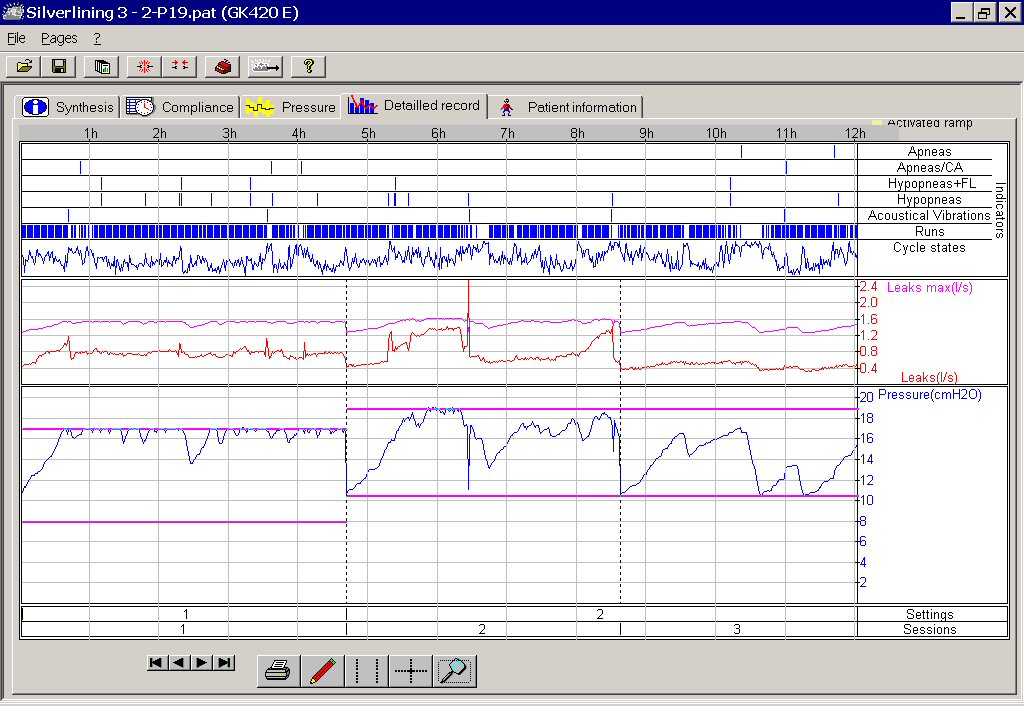
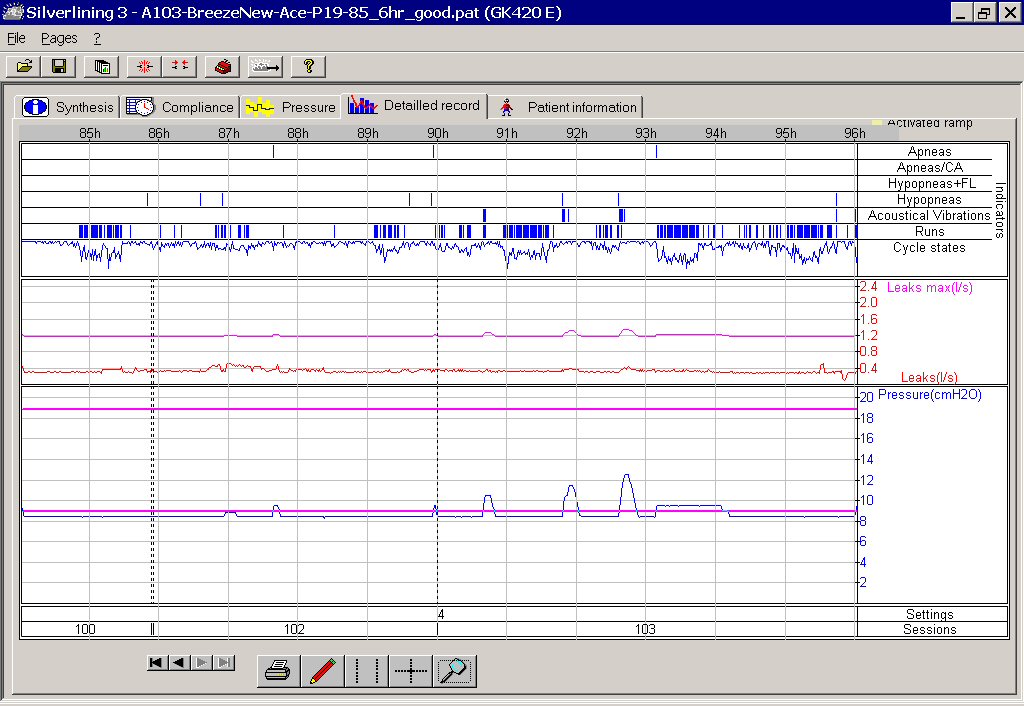
Below are a couple of pictures of the 420E in action, showing how IFL1 being on (it is "On" by default from the mfgr) didn't suit me at all. And how well things settled down after IFL1 was off. This is why, although I personally love the little 420E, it's not the autopap I'd generally recommend for new people.
Not unless they are going to use the software and are aware of what IFL1 might do with some people. And not as long as it comes from the manufacturer with IFL1 turned on. And not as long as the DME setting up a 420E for a new user doesn't know they had better check a download after the very first night or two. And not as long as the DME might not have a clue about what to look for to see if IFL1 being on by default is ok for that person.
my personal experience colors my recommendations, too. Here's some of my data with the 420E:
Three sessions (1, 2, 3) with IFL1 left ON, using range of 8 - 17 and then 10.5 - 19:
Three sessions (100,102,103) with IFL1 turned OFF, using a range of 8.5 - 19:
Hey!!! I have the definitive answer to that one!!Snoredog wrote:Okay I got it now, so the general consensus here IS then:
I believe it's called a digital rectal exam because of the one/zero answer invariably returned by this medical procedure.snoredog wrote:Why is a Digital Rectal Exam called that when it is done with an analog finger in a glove?
You must really have some reading comprehension problems.Snoredog wrote:Okay I got it now, so the general consensus here IS then:
1. SAG and other PSG's techs are always wrong and we should never rely on them for finding the correct pressure (sorry SAG some beach, by Blake Skelton).
2. We should open our autopaps up from 4cm to 20cm and just let her rip!
3. Chin straps are optional should doing that blow the top of your head off, should that happen the chin strap will hold it on so you don't lose anything.
4. Why is a Digital Rectal Exam called that when it is done with an analog finger in a glove?
You be the straight guy, I'll do the comedy.-SWS wrote:I believe it's called a digital rectal exam because of the one/zero answer invariably returned by this medical procedure.snoredog wrote:Why is a Digital Rectal Exam called that when it is done with an analog finger in a glove?
This Medical Test's Two Answers: "One" or "Zero"
The Prompting Medical Question: "Wow! How many index fingers did your hand end up with after performing a rectal exam on that really uptight patient?"
Digital... right? One/zero.
BTW, that APAP gone awry did just swimmingly with the ASV.rested gal wrote:If you're referring to the PB420E graph on page 2, I still wish I could'a sneaked in there to flip off IFL1.StillAnotherGuest wrote:The above APAP disaster
Might not have made one bit of difference for Wally. Oh, wait, you said that wasn't Wally??? I could have sworn the peaks looked tall enough to be him!
