Page 37 of 42
Posted: Mon Feb 04, 2008 11:35 pm
by Slinky
Anonymous wrote:What is "F & C" ?
F & C = typo for F & P - Fisher & Paykel, a CPAP and CPAP mask manufacturer.
Anonymous wrote:what is "date collection"?
Date collection = typo for data collection = keeps a record of your stats when the device is used, i.e. number of hours used, number of nights used, number of apneas and hypopneas that occured that night, etc.
data collection
Posted: Tue Feb 05, 2008 9:30 am
by donf
Hi folks. I've been reading these forums for a while, but this is my first posting!
Regarding the data collection on the Adapt SV. I started out in the CPAP world last spring with a Resmed APAP. Every morning I religiously checked the stats. With some tweaking of the pressures, I was able to get my AHI down to the mid-teens but no lower.
A new sleep study determined that my problem is Central Apnea and my doc put me on the Adapt SV. In yet another sleep study, the new machine put my AHI at 0.000000.... I and the doctor were deliriously happy.
Unfortunately, when I got the machine home, I learned that it DOES NOT give simple answers like the AHI for the night. It gives a bunch of stats that are totally meaningless to me.
I was successful in getting in touch with Resmed and was told that the new firmware, to be available about now, would provide those stats. I was also told that there would be no upgrade available for my machine!
Bottom line is that I think the Adapt SV is doing what it's supposed to do, but the only evidence is that my wife says I'm still not snoring.
My DME tells me that they can get me the software if the doc will just prescribe it, but I'm pushing her (on principle more than anything else) to buy the software herself and let me use it either at home or at her office.
Anyway, I was actually writing this book just to see whether anybody out there could provide an explanation of the stats that the machine provides and maybe some way to translate them to stats that would actually tell me something meaningful.
Posted: Mon Feb 18, 2008 10:01 am
by Banned
More from the fodder-file. The improved ResMed Adapt SV will be a new machine called the ReMed Adapt SV Enhanced. The 'Enhanced' may be a sticker on the new machine. Max PS will increase from the current 20cmH2O to 25cmH2O. No info on enhanced software capabilities.
Cheers
I'm not a medical professional either. In fact, my sleep-lab doc said he would never prescribe a ResMed Adapt SV for me. Some doctors really suck!
Machine: ResMed Adapt SV
Mask: Quattro FF
Humidifier: Sullivan HumidAire (Old style stand-alone)
Posted: Mon Feb 18, 2008 11:27 am
by WNJ
donf,
With my wife’s VPAP Adapt SV with ResLink, we have a “Data Management Card” (P/N: 26863) which gives an overview of the data which is captured and stored by the VPAP Adapt SV and includes information on interpreting data (includes definitions of terms, etc.)
Let me know if this would be useful and I will try to transcribe it to a post here.
(This is probably something that the DME was supposed to remove from the bundle of literature before delivering it to the end user. We also got the Clinician's Manual for the ResLink, in four languages.)
Wayne
Posted: Mon Feb 18, 2008 5:53 pm
by donf
That would be GREAT, WNJ. Any info I can get would be appreciated.
Does anybody know what kind of information you might see with the RESMED software with/without the reslink gadget?
Posted: Mon Feb 18, 2008 7:20 pm
by dsm
Just found out some info that confirms what I long believed to be the case.
The Adapt SV is a Servo Ventilation machine - uses an ancillary airline to the mask to monitor what goes on there because that is critical to being able to perform servo ventilation.
The BIPAP SV stands for Spontaneous Variable which has little to do with servo ventilation. In fact it is the Bipap Auto with an extended algorithm and was named SV for marketing reasons. It doesn't use any extra air line to sample pressure at the mask because it is just a Bilevel with the extra algorithms to extend the Auto capability.
The Bipap SV still uses the Bipap Air Valve which is a very good way of adjusting the airflow (responds quickly).
The Adapt SV uses a newly developed variable speed motor with dual impellers to control its airflow plus samples the pressure at the mask.
As with all these machines, one really has to look under the covers to figure out what the marketing info really means.
In terms of which machine suits who, I would lean to the Adapt SV as being the better machine for people with centrals & both being able to help people with OSA who are on high CMS settings. As for CSDB sufferers, am not sure.
DSM
Posted: Mon Feb 18, 2008 7:21 pm
by WNJ
donf,
From the card I mentioned:
-------------------------------
Interpreting Data
EEP (End expiratory pressure)
EEP is the pressure at the end of expiration. It is the lowest pressure delivered during a respiratory cycle.
Flow (instantaneous)
The patient flow determined by the flow generator is the total flow minus leak and mask vent flow components.
Leak
Values of leak above 30L/min indicate poor mask fit. Check the mask seal and, I f using a nasal mask, try a full face mask instead. High leak will affect treatment and compliance, and will activate the Leak Alert alarm (if enabled.)
Minute ventilation
Minute ventilation is a measure of the total volume breathed in (or out) during any 60 second period. It is calculated from respiratory rate X tidal volume. A typical range is 5-12 L/min. Minute ventilation (MV) is displayed on the VPAP Adapt SV in Treatment Screen 3.
Pressure
On Treatment Screen 1, the top right corner displays the range from minimum pressure (EEP) the maximum pressure (peak intended pressure0 when in ASV mode. This is the delivered pressure for the most recent breath. IN CPAP mode, the set pressure is displayed.
Pressure (instantaneous)
The Pressure display in the VIEW tab of the ResControl II shows the instantaneous (real-time) mask pressure.
Pressure (Inspiratory / Mean / Expiratory)
The Pressure trace displayed in the ResScan shows the inspiratory, mean and expiratory (EEP) pressure. This is the calculated delivered pressure. If it differs markedly from the pressure set on the flow generator, check that the device is functioning properly.
Pulse rate
Pulse rate data is gathered from tan oximeter connected to the ResLink and is displayed only in the ResScan after download from the SmartMedia card.
Respiratory rate
Respiratory rate is the number of breaths per minute. The displayed rate is the average of the last 5 breaths.
SpO2
SpO2 data is gathered from an oximeter connected to the ResLink. The SpO2 trace in ResScan has a red indicator line at 90%. This line makes it easy to see where the desaturations are occurring, and to connect their occurrence with apnea events.
Target ventilation
Target ventilation is the Minute ventilation that the VPAP Adapt SV is attempting to achieve. Pressure support is increased if the Minute ventilation falls below this target, and decreased if it goes above.
Tidal volume
The volume of air inspired in one breath.
-------------------
Hope this helps.
Wayne
Posted: Mon Feb 18, 2008 9:25 pm
by Banned
"Just found out some info that confirms what I long believed to be the case.
The Adapt SV is a Servo Ventilation machine - uses an ancillary airline to the mask to monitor what goes on there because that is critical to being able to perform servo ventilation.
The BIPAP SV stands for Spontaneous Variable which has little to do with servo ventilation. In fact it is the Bipap Auto with an extended algorithm and was named SV for marketing reasons. It doesn't use any extra air line to sample pressure at the mask because it is just a Bilevel with the extra algorithms to extend the Auto capability.
The Bipap SV still uses the Bipap Air Valve which is a very good way of adjusting the airflow (responds quickly).
The Adapt SV uses a newly developed variable speed motor with dual impellers to control its airflow plus samples the pressure at the mask."
That's very interesting dsm. So what does that mean for all the Doctors, RTs. DME Providers, and End Users, who have been conned by the Respironics marketing machine into thinking the Respironics BiPAP SV will help their CSA? That's gotta hurt:lol:!
Cheers
I'm not a medical professional either. In fact, my sleep-lab doc said he would never prescribe a ResMed Adapt SV for me. Some doctors really suck!
Machine: ResMed Adapt SV
Mask: Quattro FF
Humidifier: Sullivan HumidAire (Old style stand-alone)
Posted: Mon Feb 18, 2008 9:49 pm
by dsm
[quote="Banned"]
<snip>
That's very interesting dsm. So what does that mean for all the Doctors, RTs. DME Providers, and End Users, who have been conned by the Respironics marketing machine into thinking the Respironics BiPAP SV will help their CSA? That's gotta hurt:lol:!
Cheers
I'm not a medical professional either. In fact, my sleep-lab doc said he would never prescribe a ResMed Adapt SV for me. Some doctors really suck!
Machine: ResMed Adapt SV
Mask: Quattro FF
Humidifier: Sullivan HumidAire (Old style stand-alone)
Posted: Mon Feb 18, 2008 11:15 pm
by Banned
The Respironics BiPAP SV is advertised to treat Complex Sleep Apnea (OSA & CSA). If I were using a Respironics BiPAP SV my question would be, "Can a Spontaneous Variable appropriately mitigate a CSA without sampling at the mask?' Probably not. I don't think 'con' was necessarily too harsh. I do appreciate your input.
Cheers
I'm not a medical professional either. In fact, my sleep-lab doc said he would never prescribe a ResMed Adapt SV for me. Some doctors really suck!
Machine: ResMed Adapt SV
Mask: Quattro FF
Humidifier: Sullivan HumidAire (Old style stand-alone)
No It's Not
Posted: Tue Feb 19, 2008 4:18 am
by StillAnotherGuest
[quote="dsm"]Just found out some info that confirms what I long believed to be the case.
The Adapt SV is a Servo Ventilation machine - uses an ancillary airline to the mask to monitor what goes on there because that is critical to being able to perform servo ventilation.
The BIPAP SV stands for Spontaneous Variable which has little to do with servo ventilation. In fact it is the Bipap Auto with an extended algorithm and was named SV for marketing reasons. It doesn't use any extra air line to sample pressure at the mask because it is just a Bilevel with the extra algorithms to extend the Auto capability.
The Bipap SV still uses the Bipap Air Valve which is a very good way of adjusting the airflow (responds quickly).
The Adapt SV uses a newly developed variable speed motor with dual impellers to control its airflow plus samples the pressure at the mask.
As with all these machines, one really has to look under the covers to figure out what the marketing info really means.
In terms of which machine suits who, I would lean to the Adapt SV as being the better machine for people with centrals & both being able to help people with OSA who are on high CMS settings. As for CSDB sufferers, am not sure.
DSM
Posted: Tue Feb 19, 2008 4:46 am
by dsm
SAG,
Fair comment - I saw one on
http://www.cpapauction.com/ and they listed it as Spontaneous Variable - I mistakenly took that to mean that is what they were called.
http://www.cpapauction.com/browse/cpap- ... :0:91,1,:0
I agree that they do mean Servo Ventilation. Which leads me to the question how do they achieve Servo Ventilation (seriously) without an ancillary air line to the mask - I can't see how they can ?. The machine can only guess what is happeneing at the mask, n'est pas ?.
Cheers
DSM
Posted: Tue Feb 19, 2008 9:49 am
by Banned
I assumed, until now, the Respironics BiPAP SV had the ancillary sensor line. I know with my Adapt SV when I stop breathing (hold my breath) the Adapt SV starts ramping to provide much more air by my next breath. When ResMed says on a "breath-by-breath" basis, it's true. Exhalation (EEP) is fixed, but I can watch the Inhalation pressure change with each breath on the Adapts LCD. If I had serious issues with stopping breathing at night (which I do) I would be hard pressed to want to snuggle up to a Respironics BiPAP SV without any feedback from the mask.
Cheers
I'm not a medical professional either. In fact, my sleep-lab doc said he would never prescribe a ResMed Adapt SV for me. Some doctors really suck!
Machine: ResMed Adapt SV
Mask: Quattro FF
Humidifier: Sullivan HumidAire (Old style stand-alone)
Posted: Fri Feb 22, 2008 8:49 pm
by Guest
From above...the new machine will be called the "Remed' Adapt SV? Not sure if that's true or just sloppy typing. Can anyone confirm?
We Are Interested In Results
Posted: Sat Feb 23, 2008 7:00 am
by StillAnotherGuest
Banned wrote:I assumed, until now, the Respironics BiPAP SV had the ancillary sensor line. I know with my Adapt SV when I stop breathing (hold my breath) the Adapt SV starts ramping to provide much more air by my next breath. When ResMed says on a "breath-by-breath" basis, it's true. Exhalation (EEP) is fixed, but I can watch the Inhalation pressure change with each breath on the Adapts LCD. If I had serious issues with stopping breathing at night (which I do) I would be hard pressed to want to snuggle up to a Respironics BiPAP SV without any feedback from the mask.
Well, my first thought would be that where you take measurements is academic. If you know the characteristics of the machine tubing, planned leaks (mask vent rate) and the unplanned leaks are relatively constant, you could calculate everything you need to know no matter where you take the measurements. Further, the purpose of ASV is simply to supply ventilation during periods of reduction (specifically central apnea) and both machines do this quite well.
The advantage of measuring proximal airway pressure (pressure at the mask), would be that (theoretically) you could match up machine breaths to patient breaths more easily. I believe that measuring breaths at the machine is less sensitive
when there is patient effort (patient is actively particiapting in ventilation, rather than letting the machine do all the work), as shown in this
graph of pressure measurements taken in an AdaptSV circuit at patient airway (Flow 1) and machine (Flow 2):
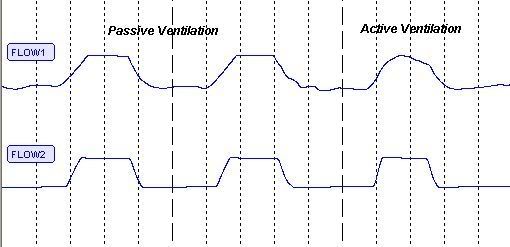
When the breath is largely from the machine, both waveforms are similar, but during periods of greater patient effort, changes are seen in the patient waveform that are not reflected in the machine waveform. So if the ASV is trying to recreate a breath pattern that closely mirrors patient effort (more like PAV technology), then this might be a better way to do that.
Now, one might ask, what value is this information? If you're asleep, having a central apnea, and the ASV is simply trying to generate a breath that is tailored not for comfort, but rather to a volume to stabilize breathing, then I'm thinking, "Who cares?" I mean, great, perhaps you can duplicate waveforms so the waveforms "look" the same, but you're ASLEEP! So is this really just another Wake comfort measure, or is there true physiological value to this?
Besides, with the newer bilevel technologies, there aren't any more square waveforms, they're all much more patient-friendly.
Again, this boils down to "what is it you're trying to fix?" If you're trying to fix CSA, you have to see that machine performance is addressing exactly that. While it may be attractive to say. "Look at that proximal patient line, that must really DO something!", you really have to see which machine fixes the underlying problem better.
This is also another good example demonstrating that the waveform out the machine is not necessarily the same as what the patient is getting, so "treating the waveform" can get you in a real rut. If the machine generates a square waveform, and patient effort is passive, then it will have a flat appearance as flow appears constant. This does not signify a flow limitation, only that the machine is delivering steady pressure.
SAG