See, here's the problem with 50 inches of snow here:
There's no place to put it.
I mean, pulling out of driveways and intersections is an adventure when there are 8-foot snowheaps on either side. You have to ease out to see anything, and it can be a little disconcerting when you're in the middle of the road and see the sanding truck bearing down on you at 90 miles an hour.
Anyway, those are great questions and should spark enough discussion to get us to the croci.
BTW, did you spend any time on CPAP? That DL should be put under the microscope.
secret agent girl wrote:”REM is astoundingly clean.” means no SDB during REM? That’s odd, isn’t SDB worse in most people during REM?
Don't forget, you were being treated (at your peak pressure) and on your side at the time, but that said (Damn!) your REM is sparkling, and this is exactly what happens in CompSAS.
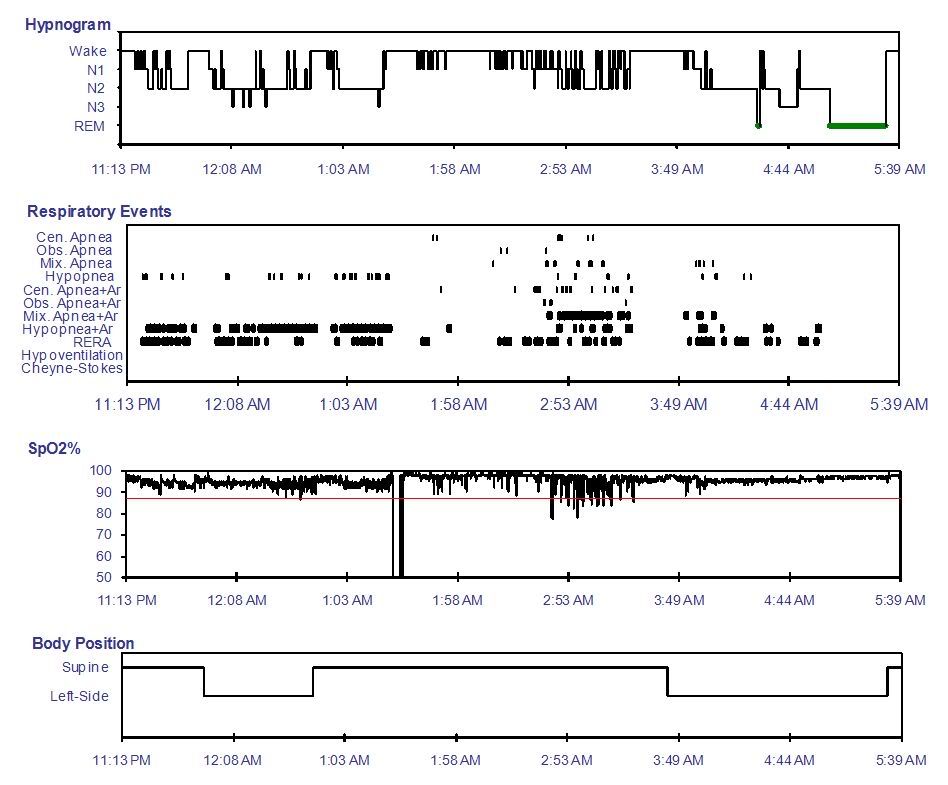

secret agent girl wrote:“The desaturations are significant enough that they really need to be treated.” and “the desaturations are generally mild as rated by the Flemons criteria.” How do these two things fit together? Isn’t xpap the only way to treat desats?
xPAP is the "best" way to treat obstructive SDB. SDB has a sliding scale of severity ("IMHO")(and apparently a few other people) that is not based exclusively on AHI:
The severity of sleep apnea can be categorized as mild, moderate, or severe on the basis of the apnea-hypopnea index. Mild sleep apnea is defined by an apnea-hypopnea index from 5 to 14, an oxygen saturation of at least 86%, and minimal daytime disability. Moderate sleep apnea is defined by an index from 15 to 30 or an oxygen saturation of 80% to 85% and significant work or social dysfunction due to drowsiness and loss of concentration. Severe sleep apnea is defined by an index greater than 30 or an oxygen saturation of 79% or less and incapacitation due to the sleep disorder.
Definitions
This gives a number of combinations, so again, my point is, perhaps the decision to treat is not always crystal-clear in some patients. If a patient desats to 60%, has hypertension and a history of falling-asleep-at-the-wheel autombile accidents, the decision is easy-- "If you don't use CPAP, you'll be dead in five years. Pay the receptionist on the way out."
I offer this to try to explain why you (and others) feel worse with treatment and promote an understanding of the compliance issue.
That said, (AAAAHHHHHHH!!!) eventually we'll post some epochs to show what specifically what can be addressed in your case to try to fix SBD and (hopefully) improve sleep. I think the general philosophy should be low-level pressure and whatever adjunct necessary for comfort.
secret agent girl wrote:Can it be determined what causes “arousals progress to wake” and “sleep efficiency [to be] abysmal across the board”? What might it be? I think I’ve understood you to say that it would be treated with drugs--sleeping pills?
Sleep aids are one solution. However, I would strongly recommend that you get an 8-week plan of what and where you want to go with that with your physician. You can use some of them long-term safety. I also think you need a heavy dose of CBT (insomnia discussion to follow)(as well as sleep hygiene discussion).
Blanket Judgement Statement:
Perimenopausal women have bad sleep.
Another one of those Gifts from God.
Gotta run.
LOL.
Whoops!
Gotta shovel first.
Lemme tell ya, buying new shoes is like washing your car in re: predicting the weather.
The Big Guy certainly has a great sense of humor!!









