







This is the first one of the two I want to summarize; it's from the medical journal Chest which carried many respiratory articles. OK, since this is a medical journal I wonder if you can read it free; but public libraries usually have a Proquest account and you can read the full text there.
The following is a summarization of the publication and does not represent my views.
Title of publication: Bench Evaluation of Flow Limitation Detection by Automated Continuous Positive Airway Pressure Devices
by Frederic Lofaso, Gillbert Desmarais, Karl Leroux, VIncent Zale, Redouane Fodil, Daniel Isabey, Bruno Louis.
Conflict of interest: All writers declared they have no conflict of interest.
Summarization of Content:
Flattened respiratory waves (as you can see below) are commonly recognized as a predictor of subtle obstruction and since they herald snoring, hyponea and apnea, CPAP should intervene. Clinically it has been proven CPAP level that removes such flattening improves sleep quality. So how APAPs do in detecting and removing APAP?
APAPs tested:
- GoodKnight 418P
- GoodKnight 420E
- ResMed Autoset Spirit
- Respironics Remstar Auto
- Breas PV10i
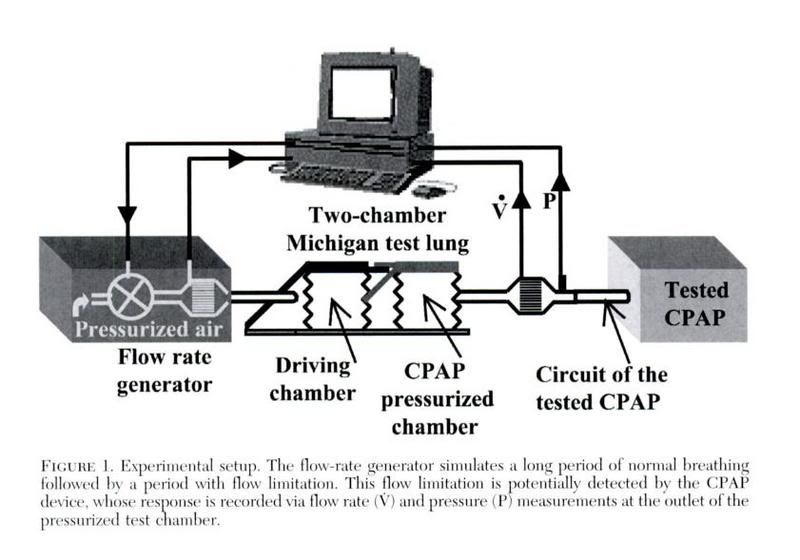
A http://www.michiganinstruments.com/resp-ttl-dual.htm provides the respiratory wave; it is then modified by a flow rate generator which modify waves to the desired form. This modified respiratory wave is then used as the input of an APAP and its output pressure is modified.
Two sets of waves are produced:
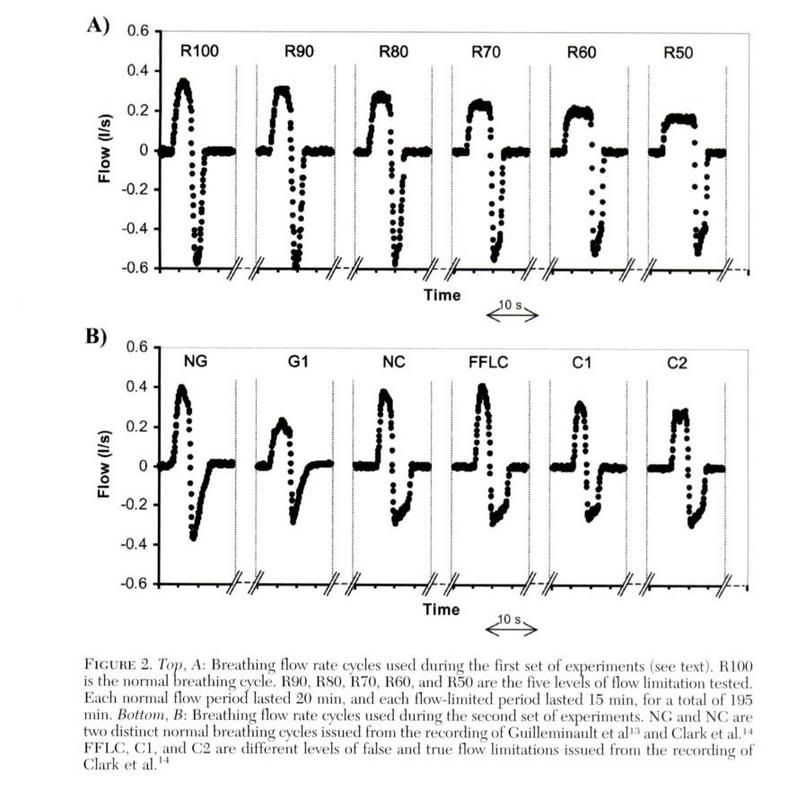
A: These are simulated flattened waves. The number after the R is the height of the wave NOT flattened, so an R100 is equal to a normal breath wave. The testing waves are run for 15 mins, and 20 mins of normal waves are applied between tests.
B: NG: Normal wave as described by Dr. G.
G1: Flow limited wave as described by Dr G.
NC: Normal wave as described by Dr C.
FFLC: False Flow limitation cycle described by Dr C.
C1, C2: Flow limited waves as described by Dr C.
Otherwise the time is same as A.
Results:
Brea: After 5 minutes, the set was auto-triggered to rise to maximum pressure within 340s.
Respironics: Doesn't seem to respond to the waves; pressure increased by 1.4cmH2O over 160s and goes back to initial in 60s, cycled every 540s even with flattened waves.
Others: seemed to respond better but unable to detect all flattened waves. See the following picture:
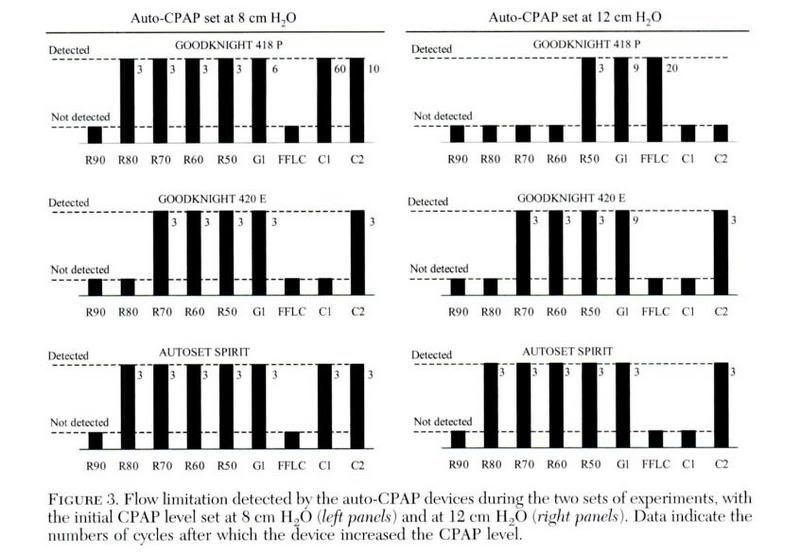
However, ResMed and the GoodKnights differ in how they apply pressure; RedMed increased pressure steadily up to the maximum, while the GoodKnights increased by a 0.3cmH2O step after they detected the flattened wave.
Some discussions from the writers:
Resmed shown the best sensitivity but that does not mean the best since doctors' strategy differ. Overlap occurs normal people and people with obstruction; normal people might have flattened waves; and people with apnea does not consistently exhibit flattened waves. Hence, over- and hyper-sensitivity might be a problem for any APAP.
Future APAPs would more likely to be customizable to different patient subtypes, and manufacturers should disclose their algorithms so that doctors may tweak the APAPs for patients, especially when different APAPs, using the same flow limtation algorithm, differs so much in sensitivity and response...
_________________
CPAPopedia Keywords Contained In This Post (Click For Definition): 420E, respironics, resmed, CPAP, auto, APAP



