REM stage sleep is hard to determine just by looking at the cpap machine software. One has to look at the normal time frames where REM seems to occur and try to correlate them with similar time frame on the software reports.
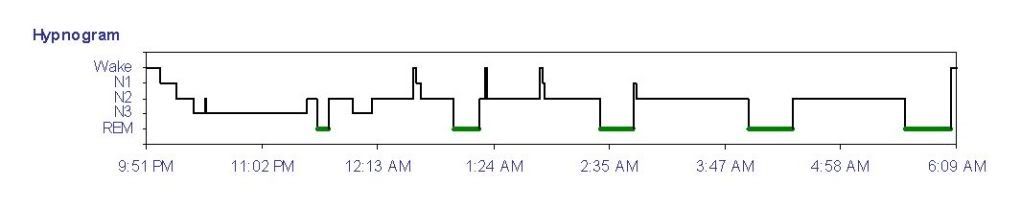
Maybe this hypnogram will make it a bit easier. Generally (remember this isn't an absolute) we see the first REM stage around 90 to 120 minutes into sleep...and as the night goes one it occurs more frequently and lasts longer until we reach the we hours of the morning where we can see a lot more REM.
Also remember that when we have frequent awakenings...those awakenings are going to mess with the normal sleep cycles...that's why we want awakenings to a minimum...we feel like crap because we don't get the right % of sleep stages that are needed for the restorative powers of sleep to work its magic.
Have you got a copy of your sleep study? Often it will mention the various sleep stages along with sleep positions and it is pretty easy to spot if supine sleeping or REM sleep seems to be a factor in AHI. They aren't always a factor though. Some people won't see much of a change in either the number of events or pressure needs with either. It is common though...but not a 100% certainty that everyone in the whole world will have horrible numbers of apnea events with supine sleeping or need massive pressure increases to deal with them.
My feelings have always been....good sleep is primary goal and if I happened to have worse OSA or higher pressure needs supine sleeping (or same argument with REM stage sleep worse OSA) and I just don't want to or can't limit myself to side sleeping....hey, that's why we have the machines anyway...let the machine do its job.
If more pressure is needed for part of the night...use auto adjusting pressures. If auto adjusting pressures disrupt sleep...compromise maybe. I would compromise if auto adjusting pressures created a problem for me like with sleep disruptions or higher pressures caused aerophagia.. I am lucky...they don't bother me but I know some people the auto adjusting features are a problem.
If a machine is properly adjusted...the machine does its job preventing events no matter when or where or why they occur and I don't really care if it prevented 1 event or 100 events as long as they were prevented.
fredn wrote:Let me ask .... if it is even this cut and dry ... does "auto leveling" help to prevent an increasing string of obstructions by incrementally increasing pressure and in turn getting to a high enough pressure to stop them.
Yes, if those obstructions seem to require a little more pressure than initially is being delivered..that's the "job" of the machine when in auto adjusting mode. The minimum pressure that is being used is real important though. These machines don't go from 5 to 10 or 10 to 15 or whatever in a blink of an eye in response to an obstruction that may need more pressure.
Remember the triggers are snores and flow limitations and not the actual obstructive event...it's the level of flow limitation that remains after an obstructive event has cleared that machine looks at and says...hmmm maybe we need a little more pressure so here I go...
fredn wrote:Does that reasoning sound decent?
Yes, it is sound reasoning. Your choices are.. use auto adjusting mode with a minimum pressure that does a decent job most of the night but is close enough to what maybe might be needed at other times during the night that it can get there quickly enough...
or
you can use cpap mode and maybe use a constant pressure a little higher all night in hopes that the little higher pressure all night is sufficient to maintain an open airway with minimal tissue collapse.
This principle applies to apap mode or bilevel auto mode. Only thing with bilevel is we get to have the comfort of EPAP and IPAP difference making it easier to exhale. The basic logic is pretty much the same...minimum APAP and EPAP minimum needs to be a good starting point.
Now I have done extensive experiments with straight bilevel mode on my BiPap machine...fixed EPAP and IPAP. Pretty darn good results because I think the higher IPAP helps EPAP (overall pressure average is higher than when using APAP mode) a lot by better job holding the airway open and thus preventing the need for the greater pressures in the wee hours of the morning. I might have a random little cluster pop up that likely if I was in auto mode would raise the pressure but overall it doesn't happen often and the clusters aren't huge in numbers. This is where I would compromise if I happened to be sensitive to pressure variations.
I would accept a random small cluster as acceptable result...AHI of 0.0 has never been my goal.
Good quality sleep with minimal sleep disruptions and feeling decent the next day has always been my primary goal.
AHI of 0.0 is real easy for me to get if I never go to REM sleep.. If I have a lot of fragmented sleep my AHI is nothing but then I simply don't sleep well and I feel horrible the next day.
Don't get me wrong..it's not that I totally ignore the AHI and all that but I don't base my "success" on a number. Numbers often don't tell the whole story. I discovered a long time ago that if I broke up my "clusters" that I felt better the next day...more rested.
I think that in my case those little clusters likely caused some sort of mini arousal (that I may or may not have remembered) and thus messed with my sleep cycles and I simply was getting enough Deep Sleep and REM sleep where most of the restorative work is accomplished. This is why one of my first questions to anyone complaining of feeling like crap despite a nice report on paper is going to be "is your sleep fragmented, waking up often, tossing and turning (because if they remember tossing and turning a lot then I know they were awake) "
You could probably find a straight cpap mode set of settings that will do an acceptable job...or straight bilevel mode that would do an acceptable job...you might or might not have to make a compromise.
Me....since auto adjusting mode doesn't seem to bother me at all...I choose to just let the machine do the work it is designed to do.
I feel just as well rested in auto mode as I do in straight mode. If I didn't I would use the mode that let me feel the best.
Since each person can respond differently to auto mode in any machine...then auto mode may not be for everyone.
There is no right or wrong...just whichever works best for the individual.
I may have to RISE but I refuse to SHINE.
If you want to try the Eclipse mask and want a special promo code to get a little off the price...send me a private message.









