1. The issue of responding
after an apnea is identified is only relevant to automatic pressure machines. On fixed pressure machines, the pressure is fixed and if a person needs a pressure of 12 to keep them from having most of their apnea, that's what they'll have. Their pressure is independent of events.
2. Automatic machines have to distinguish obstructive apneas - which justify a rise in pressure - from non-obstructives ones, that do not need raise in pressure.
3. The companies who make automatic machines go about this identification process in different ways.
Resmed's Auto Set Algorithm is described here:
http://www.resmed.com/en-au/clinicians/ ... clinicians
And here:
http://www.talkaboutsleep.com/sleep-dis ... chat.htm#6
ResMed's Simon J.P. Johnson wrote: The A10 algorithm increases pressure in response to Flow Limitation, Snore, and Apnea up to 10cm H2O. Above 10cm H2O, pressure response to Flow Limitation and Snore continues, but there is no response to Apnea. AutoSet Spirit and AutoSet T do not differentiate between obstructive and central apneas. Increasing pressures above 10cm H2O in response to apnea can lead to "runaway" central apneas,
This algorithm is still in use in the S8 machines.
If a person has apneas, but no snores or flow limitations above a 10 cwm,
then a Resmed may not be the best machine for treatment. However, the majority of people have flow limitation and snores as well as apneas, and Resmed think it is safe enough to stop at 10.
Respironics identity apneas /hypopneas that do not respond to pressure, and then drop the pressure back down after having raised it too much.
Respironcs wrote:
Above 8 cmH2O pressure, the pressure increase for sustained apneas/hypopneas is limited to 3 cmH2O above the pressure setting at the onset of the apnea/hypopnea sequence. The pressure setting at the onset of the sequence is called the "Onset Pressure." The pressure 3 cmH2O above the "Onset Pressure" is called the "NRAH Threshold." "NRAH" is an acronym for "Non-Responsive Apnea/Hypopnea."
<snip>
When the device encounters a non-responsive apnea or hypopnea, it will decrease pressure by 2 cmH2O and hold the pressure for 15 minutes. During this 15-minute "NRAH-hold" period, the pressure will be changed only in response to detection of a sequence of vibratory snore events. The reason for this increase in pressure followed by a decrease in pressure when an apnea/hypopnea is not responsive is to allow the device to respond appropriately to an event that is not treatable by increases in pressure, such as a central apnea
.
Emphasis added by me.
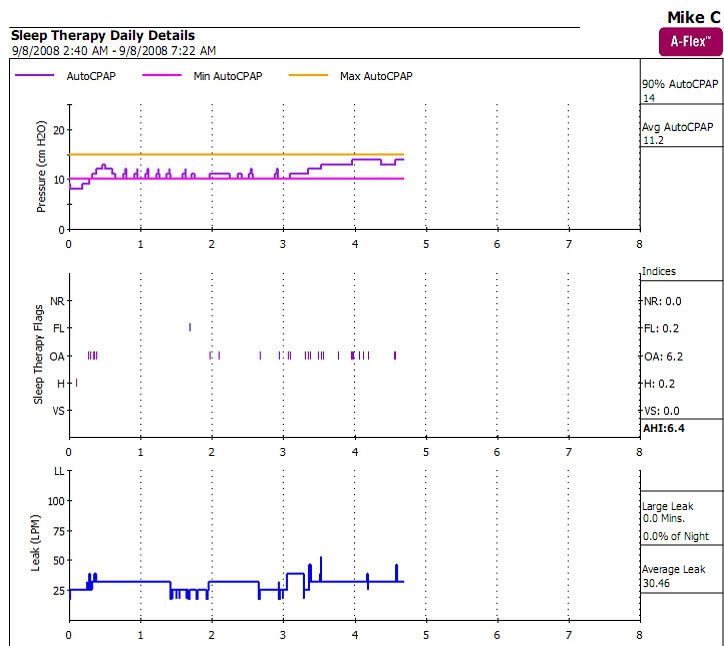
Your machine is raising the pressure, Mike, because your apneas are responsive to those pressure raises. You do not not sustained apneas that are not responding the rise in pressure.
On
Puritan Bennett automatic machines, you can tell the machine what the maximum pressure will be in response to apnea - the default is 10, but it can be set both higher or lower. The machine is also capable of identifying heartbeat oscillations in the air flow. Their existence indicates that the airway is open, and therefore the machine will not raise pressure in response to apneas accompanied by cardiogenic oscillations - no matter what pressure they occur at.
All of these algorithms will raise pressure as higher than 10 if they run into flow limitation or snores.
O.
Edited some typos....And now here is my secret, a very simple secret; it is only with the heart that one can see rightly, what is essential is invisible to the eye.
Antoine de Saint-Exupery
Good advice is compromised by missing data
Forum member Dog Slobber Nov. 2023