deltadave wrote:robysue wrote:Are you saying:
Arousals lead to aerophagia and aerophagia leads to decreased sleep efficiency due to additional wakes caused by the aerophagia?
'Zactly!
and
deltadave wrote:
ignorant1 wrote:That begs the question of if that would cause a change in thoracic pressure, enough to overcome the LES “seal” against the increased respiratory tract pressure from xPAP?
The pressure required to open a normally functioning closed LES is about 25 - 33 cmH2O. Clearly, the unpredictability of aerophagia requires there to be other factors underfoot.
Keep in mind that the easiest way to relax an LES is to simply swallow. (As an aside, I would also offer that the easiest way to elicit a swallow during sleep is to generate an arousal, which may be the mechanism of the PLM point. It's not PLMs, it's the subsequent arousals).
The idea that arousals (of any sort?) lead to swallowing which leads to aerophagia which leads to more wakes and less sleep efficiency (and more swallowing? and more aerophagia?) makes some sense to me---at least in the sense of explaining why I have so much more aerophagia on night's that starts out restless to begin with. I do know that I tend to swallow whenever I first wake up. So it makes sense that even an arousal (for whatever reason) could also lead to reflexive swallowing.
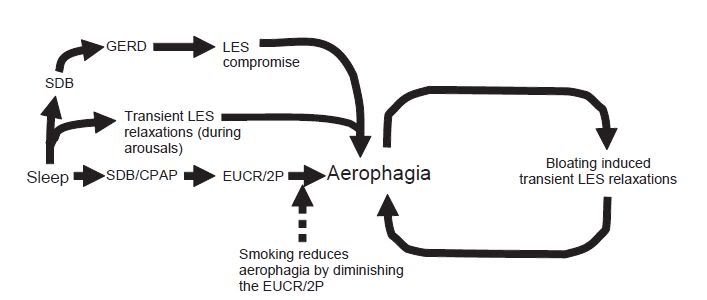
But this also seems to imply that there's a nasty feedback loop going on here as well:
Arousals -> Swallowing -> Aerophagia -> Discomfort -> Awakenings -> More Swallowing -> More Aerophagia -> More Discomfort -> and so on until it's morning and the stomach is rock hard and/visibly distended with air.
Any ideas on how to effectively stop the feedback loop once it has gotten started?
Last night's the perfect example: I went to bed quite comfortable with absolutely no stomach problems at all. Got to sleep with no problems and no aerophagia discomfort. Startled myself awake from a dream (it was not a good dream), but there's no evidence in the data that the wake was triggered by an apnea or hypopnea: The wake was somewhere around 20 or 30 minutes after CA. There is a flow limitation around the time of that first wake. Drifting back to sleep wasn't easy---I had a 20-40 minute long period of drifting in/out sleep if I'm recalling things with any accuracy. During that restless period, there is a cluster of three OAs. I don't remember any aerophagia during that first restless period: The brain was having some trouble shutting up and there were some rainout problems and my lips were being bothered by the pillows and the exhaust flow from the mask. About an hour after those 3 OAs, I woke up with a touch of aerohpagia. And during the rest of the night, I had several more wakes (and who knows how many arousals), and each time I woke, the aerophagia was worse. By morning, my stomach and esophagus were both feeling rock hard .....