







On the contrary, in looking back over the previous opus on Bev, it is seen that she presents very typically for N. She gave a history of sleep paralysis, auditory and visual hallucinations, severe and persistent EDS in the face of seemingly effective PAP therapy, severely fragmented sleep and admitted to cataplexy.-SWS wrote:While she needs a sleep study to test for the possibility of N, she would in all likelihood presents atypically for N, even during an MSLT.
The only remaining variable was whether or not there was sleep-onset REM, which was why I wanted the sleep studies to carefully review with my own eyeballs.
And indeed, 4.0 minutes into the 8/31 study came these:
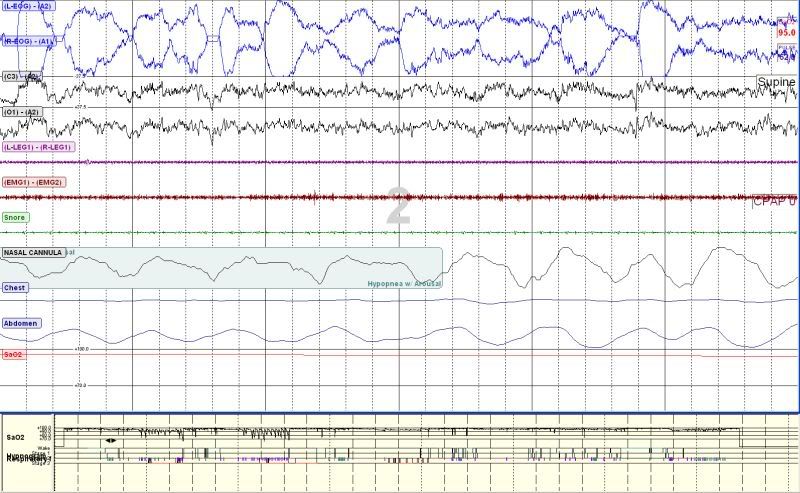
For those not in the know, the first two channels (or "squiggly lines" as we say in the business) are "REMs". The technician scored this epoch as Stage 2.
SAG

